Copyright © 2015 Bert N. Langford (Images may be subject to copyright. Please send feedback)
Welcome to Our Generation USA!
Human Sexuality
Click here for the Web Page "Feminism"
Click here for the Web Page "Nature"
Human Sexuality
YouTube Video: The Many Faces of Human Sexuality (By The World Science Festival)
Human sexuality is the capacity of humans to have erotic experiences and responses. A person's sexual orientation can influence their sexual interest and attraction for another person.
Sexuality may be experienced and expressed in a variety of ways; including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. These may manifest themselves in biological, physical, emotional, social, or spiritual aspects.
The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual response cycle and the basic biological drive that exists in all species.
Physical and emotional aspects of sexuality include bonds between individuals that is expressed through profound feelings or physical manifestations of love, trust, and care. Social aspects deal with the effects of human society on one's sexuality, while spirituality concerns an individual's spiritual connection with others. Sexuality also affects and is affected by cultural, political, legal, philosophical, moral, ethical, and religious aspects of life.
Interest in sexual activity typically increases when an individual reaches puberty. Opinions differ on the origins of an individual's sexual orientation and sexual behavior. Some argue that sexuality is determined by genetics; some believe it is molded by the environment, and others argue that both of these factors interact to form the individual's sexual orientation.
This pertains to the nature versus nurture debate. In the former, one assumes that the features of a person innately correspond to their natural inheritance, exemplified by drives and instincts; the latter refers to the assumption that the features of a person continue to change throughout their development and nurturing, exemplified by ego ideals and formative identifications.
Genetic studies work on the premise that a difference in alleles corresponds to a variation in traits among people.In the study of human chromosomes in human sexuality, research has shown that "ten percent of the population has chromosomal variations that do not fit neatly into the XX-female and XY-male set of categories".
Evolutionary perspectives on human coupling, reproduction and reproduction strategies, and social learning theory provide further views of sexuality.
Socio-cultural aspects of sexuality include historical developments and religious beliefs. Examples include Jewish views on sexual pleasure within marriage and some views of other religions on avoidance of sexual pleasures. Some cultures have been described as sexually repressive. The study of sexuality also includes human identity within social groups, sexually transmitted infections (STIs/STDs), and birth control methods.
Click on any of the following Hyperlinks for Further Amplification:
Sexuality may be experienced and expressed in a variety of ways; including thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. These may manifest themselves in biological, physical, emotional, social, or spiritual aspects.
The biological and physical aspects of sexuality largely concern the human reproductive functions, including the human sexual response cycle and the basic biological drive that exists in all species.
Physical and emotional aspects of sexuality include bonds between individuals that is expressed through profound feelings or physical manifestations of love, trust, and care. Social aspects deal with the effects of human society on one's sexuality, while spirituality concerns an individual's spiritual connection with others. Sexuality also affects and is affected by cultural, political, legal, philosophical, moral, ethical, and religious aspects of life.
Interest in sexual activity typically increases when an individual reaches puberty. Opinions differ on the origins of an individual's sexual orientation and sexual behavior. Some argue that sexuality is determined by genetics; some believe it is molded by the environment, and others argue that both of these factors interact to form the individual's sexual orientation.
This pertains to the nature versus nurture debate. In the former, one assumes that the features of a person innately correspond to their natural inheritance, exemplified by drives and instincts; the latter refers to the assumption that the features of a person continue to change throughout their development and nurturing, exemplified by ego ideals and formative identifications.
Genetic studies work on the premise that a difference in alleles corresponds to a variation in traits among people.In the study of human chromosomes in human sexuality, research has shown that "ten percent of the population has chromosomal variations that do not fit neatly into the XX-female and XY-male set of categories".
Evolutionary perspectives on human coupling, reproduction and reproduction strategies, and social learning theory provide further views of sexuality.
Socio-cultural aspects of sexuality include historical developments and religious beliefs. Examples include Jewish views on sexual pleasure within marriage and some views of other religions on avoidance of sexual pleasures. Some cultures have been described as sexually repressive. The study of sexuality also includes human identity within social groups, sexually transmitted infections (STIs/STDs), and birth control methods.
Click on any of the following Hyperlinks for Further Amplification:
- Nature-versus-nurture
- Biological and physiological aspects
- Psychological aspects
- Sexuality and age
- Sociocultural aspects
- Sexual behavior
- See also
Beauty Salons
YouTube Video: How to Pick the Right Beauty Salon
Pictured: LEFT: Hair salon styling floor; RIGHT: Facials may include the use of a facial mask. (By Sérgio (Savaman) Savarese – Flickr)

A beauty salon or beauty parlor (beauty parlour) (or sometimes beauty shop) is an establishment dealing with cosmetic treatments for men and women.
Other variations of this type of business include hair salons and spas.
There is a distinction between a beauty salon and a hair salon and although many small businesses do offer both sets of treatments; beauty salons provide more generalized services related to skin health, facial aesthetic, foot care, nail manicures, aromatherapy, — even meditation, oxygen therapy, mud baths, and many other services.
Click on any of the following hyperlinks for amplification:
Other variations of this type of business include hair salons and spas.
There is a distinction between a beauty salon and a hair salon and although many small businesses do offer both sets of treatments; beauty salons provide more generalized services related to skin health, facial aesthetic, foot care, nail manicures, aromatherapy, — even meditation, oxygen therapy, mud baths, and many other services.
Click on any of the following hyperlinks for amplification:
Birth Control
YouTube Video: Female Birth Control Options | Family Planning
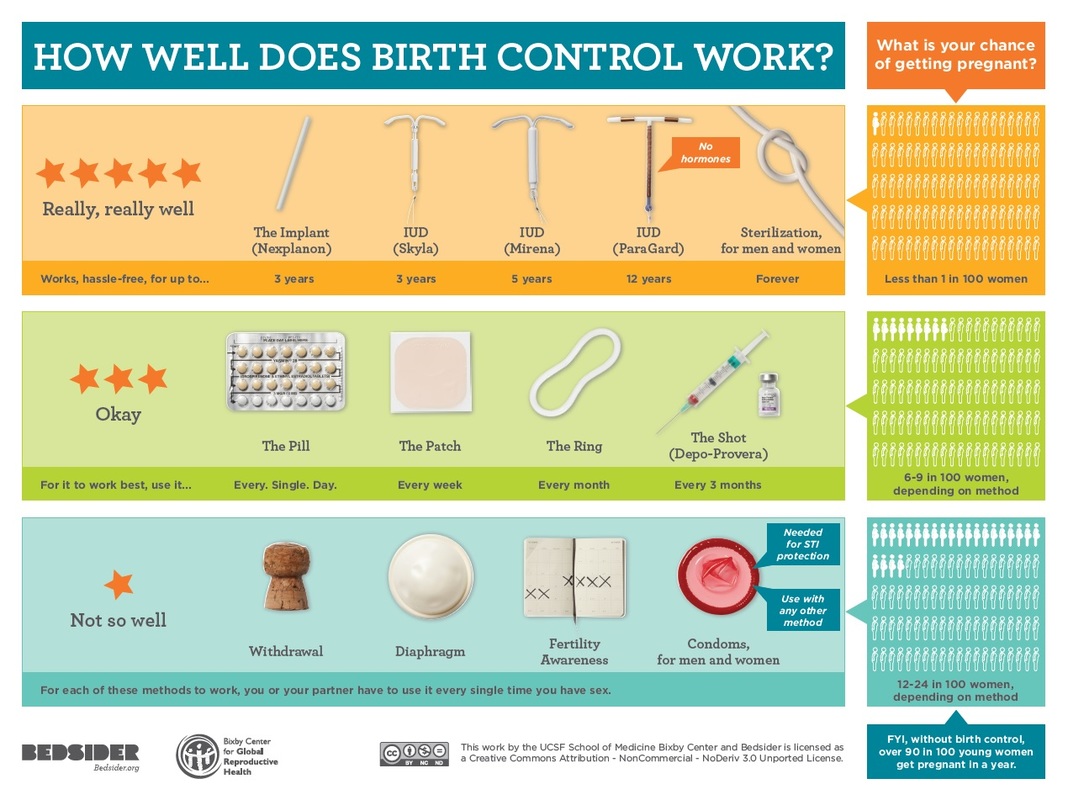
Pictured: Comparison of Effectiveness of Birth Control Methods as offered by the Women's Community Clinic
Birth control, also known as contraception and fertility control, are methods or devices used to prevent pregnancy.
Planning, making available, and use of birth control is called family planning. Birth control methods have been used since ancient times, but effective and safe methods only became available in the 20th century.
Some cultures limit or discourage access to birth control because they consider it to be morally, religiously, or politically undesirable.
The most effective methods of birth control are sterilization by means of vasectomy in males and tubal ligation in females, intrauterine devices (IUDs), and implantable birth control.
This is followed by a number of hormone based methods including oral pills, patches, vaginal rings, and injections.
Less effective methods include physical barriers such as condoms, diaphragms and birth control sponges and fertility awareness methods.
The least effective methods are spermicides and withdrawal by the male before ejaculation.
Sterilization, while highly effective, is not usually reversible; all other methods are reversible, most immediately upon stopping them.
Safe sex, such as with the use of male or female condoms, can also help prevent sexually transmitted infections.
Emergency birth control can prevent pregnancy in the few days after unprotected sex. Some regard not having sex as birth control, but abstinence-only sex education may increase teenage pregnancies when offered without birth control education, due to non-compliance.
In teenagers, pregnancies are at greater risk of poor outcomes. Comprehensive sex education and access to birth control decreases the rate of unwanted pregnancies in this age group.
While all forms of birth control may be used by young people, long-acting reversible birth control such as implants, IUDs, or vaginal rings are of particular benefit in reducing rates of teenage pregnancy.
After the delivery of a child, a woman who is not exclusively breastfeeding may become pregnant again after as few as four to six weeks. Some methods of birth control can be started immediately following the birth, while others require a delay of up to six months. In women who are breastfeeding, progestin-only methods are preferred over combined oral birth control pills. In women who have reached menopause, it is recommended that birth control be continued for one year after the last period.
About 222 million women who want to avoid pregnancy in developing countries are not using a modern birth control method.
Birth control use in developing countries has decreased the number of deaths during or around the time of pregnancy by 40% (about 270,000 deaths prevented in 2008) and could prevent 70% if the full demand for birth control were met.
By lengthening the time between pregnancies, birth control can improve adult women's delivery outcomes and the survival of their children.
In the developing world women's earnings, assets, weight, and their children's schooling and health all improve with greater access to birth control.
Birth control increases economic growth because of fewer dependent children, more women participating in the workforce, and less use of scarce resources.
Planning, making available, and use of birth control is called family planning. Birth control methods have been used since ancient times, but effective and safe methods only became available in the 20th century.
Some cultures limit or discourage access to birth control because they consider it to be morally, religiously, or politically undesirable.
The most effective methods of birth control are sterilization by means of vasectomy in males and tubal ligation in females, intrauterine devices (IUDs), and implantable birth control.
This is followed by a number of hormone based methods including oral pills, patches, vaginal rings, and injections.
Less effective methods include physical barriers such as condoms, diaphragms and birth control sponges and fertility awareness methods.
The least effective methods are spermicides and withdrawal by the male before ejaculation.
Sterilization, while highly effective, is not usually reversible; all other methods are reversible, most immediately upon stopping them.
Safe sex, such as with the use of male or female condoms, can also help prevent sexually transmitted infections.
Emergency birth control can prevent pregnancy in the few days after unprotected sex. Some regard not having sex as birth control, but abstinence-only sex education may increase teenage pregnancies when offered without birth control education, due to non-compliance.
In teenagers, pregnancies are at greater risk of poor outcomes. Comprehensive sex education and access to birth control decreases the rate of unwanted pregnancies in this age group.
While all forms of birth control may be used by young people, long-acting reversible birth control such as implants, IUDs, or vaginal rings are of particular benefit in reducing rates of teenage pregnancy.
After the delivery of a child, a woman who is not exclusively breastfeeding may become pregnant again after as few as four to six weeks. Some methods of birth control can be started immediately following the birth, while others require a delay of up to six months. In women who are breastfeeding, progestin-only methods are preferred over combined oral birth control pills. In women who have reached menopause, it is recommended that birth control be continued for one year after the last period.
About 222 million women who want to avoid pregnancy in developing countries are not using a modern birth control method.
Birth control use in developing countries has decreased the number of deaths during or around the time of pregnancy by 40% (about 270,000 deaths prevented in 2008) and could prevent 70% if the full demand for birth control were met.
By lengthening the time between pregnancies, birth control can improve adult women's delivery outcomes and the survival of their children.
In the developing world women's earnings, assets, weight, and their children's schooling and health all improve with greater access to birth control.
Birth control increases economic growth because of fewer dependent children, more women participating in the workforce, and less use of scarce resources.
Body-Building Contests
YouTube Video: Bodybuilding Motivation -Phil Heath Mr. Olympia 2015
Pictured: LEFT: Phillip Heath, Mr. Olympia 2014; RIGHT: Juliana Malacarne, Ms. Olympia 2014

Bodybuilding is the use of progressive resistance exercise to control and develop one's musculature.
An individual who engages in this activity is referred to as a bodybuilder. In competitive amateur and professional bodybuilding, bodybuilders appear in lineups doing specified poses, and later perform individual posing routines, for a panel of judges who rank competitors based on criteria such as symmetry, muscularity and conditioning.
Bodybuilders prepare for competition through a combination of dehydration, fat loss, oils, carb loading to achieve maximum vascularity, and tanning (or tanning lotions) which make their muscular definition more distinct.
Well-known bodybuilders include Charles Atlas, Steve Reeves, Reg Park, Arnold Schwarzenegger, Juliana Malacarne, Dana Lynn Bailey and Lou Ferrigno.
The winner of the annual IFBB Mr. Olympia contest is generally recognized as the world's top male professional bodybuilder. The title is currently held by Phil Heath of the United States.
The winner of the Women's Physique portion of the competition is widely regarded as the world's top female professional bodybuilder. The 2015 title is currently held by Juliana Malacarne, a Brazilian-born American IFBB Pro fitness and figure competitor and Ladies All-Star Wrestling Professional.
Since 1950, the NABBA Universe Championships has been considered the top amateur bodybuilding contest with many notable winners such as Steve Reeves, Bill Pearl, Reg Park, Arnold Schwarzenegger and Lee Priest.
An individual who engages in this activity is referred to as a bodybuilder. In competitive amateur and professional bodybuilding, bodybuilders appear in lineups doing specified poses, and later perform individual posing routines, for a panel of judges who rank competitors based on criteria such as symmetry, muscularity and conditioning.
Bodybuilders prepare for competition through a combination of dehydration, fat loss, oils, carb loading to achieve maximum vascularity, and tanning (or tanning lotions) which make their muscular definition more distinct.
Well-known bodybuilders include Charles Atlas, Steve Reeves, Reg Park, Arnold Schwarzenegger, Juliana Malacarne, Dana Lynn Bailey and Lou Ferrigno.
The winner of the annual IFBB Mr. Olympia contest is generally recognized as the world's top male professional bodybuilder. The title is currently held by Phil Heath of the United States.
The winner of the Women's Physique portion of the competition is widely regarded as the world's top female professional bodybuilder. The 2015 title is currently held by Juliana Malacarne, a Brazilian-born American IFBB Pro fitness and figure competitor and Ladies All-Star Wrestling Professional.
Since 1950, the NABBA Universe Championships has been considered the top amateur bodybuilding contest with many notable winners such as Steve Reeves, Bill Pearl, Reg Park, Arnold Schwarzenegger and Lee Priest.
Female Cosmetics
YouTube Video: Top 40 Foto Amazing Before and After makeup transformation by Goar Avetisyan
YouTube Video: STEP BY STEP GUIDE TO APPLYING EYELINER ON HOODED EYES | TECHNIQUE TUESDAY
YouTube Video: TOP 10 MAKEUP MISTAKES 2021 | NINA UBHI
Pictured: LEFT: Skillful blending of several effects: eyebrow plucking, simple black eye liner; good choice of lipstick color; subtle use of rouge (By lukeisback.com)

Cosmetics, also known as make-up, are care substances used to enhance the appearance or odor of the human body. They are generally mixtures of chemical compounds, some being derived from natural sources (such as coconut oil) and some being synthetics.
In the U.S., the Food and Drug Administration (FDA), which regulates cosmetics, defines cosmetics as "intended to be applied to the human body for cleansing, beautifying, promoting attractiveness, or altering the appearance without affecting the body's structure or functions." This broad definition includes any material intended for use as a component of a cosmetic product. The FDA specifically excludes soap from this category.
Cosmetics are intended to be applied externally. They include but are not limited to products that can be applied to the face: skin-care creams, lipsticks, eye and facial makeup, towelettes, and colored contact lenses; to the body:deodorants, lotions, powders, perfumes, baby products, bath oils, bubble baths, bath salts, and body butters; to the hands/nails: fingernail and toe nail polish, and hand sanitizer; to the hair: permanent waves, hair colors, hair sprays and gels.
A subset of cosmetics is called "make-up", refers primarily to products containing color pigments that are intended to alter the user’s appearance. Many manufacturers distinguish between decorative cosmetics and care cosmetics.
Cosmetics that are meant to be used on the face and eye area are usually applied with a brush, a makeup sponge, or the fingertips.
Most cosmetics are distinguished by the area of the body intended for application.
The Types of Cosmetics follow:
Cosmetics can be also described by the physical composition of the product. Cosmetics can be liquid or cream emulsions; powders, both pressed and loose; dispersions; and anhydrous creams or sticks.
Makeup remover is a product used to remove the makeup products applied on the skin. It cleans the skin before other procedures, like applying bedtime lotion.
In the U.S., the Food and Drug Administration (FDA), which regulates cosmetics, defines cosmetics as "intended to be applied to the human body for cleansing, beautifying, promoting attractiveness, or altering the appearance without affecting the body's structure or functions." This broad definition includes any material intended for use as a component of a cosmetic product. The FDA specifically excludes soap from this category.
Cosmetics are intended to be applied externally. They include but are not limited to products that can be applied to the face: skin-care creams, lipsticks, eye and facial makeup, towelettes, and colored contact lenses; to the body:deodorants, lotions, powders, perfumes, baby products, bath oils, bubble baths, bath salts, and body butters; to the hands/nails: fingernail and toe nail polish, and hand sanitizer; to the hair: permanent waves, hair colors, hair sprays and gels.
A subset of cosmetics is called "make-up", refers primarily to products containing color pigments that are intended to alter the user’s appearance. Many manufacturers distinguish between decorative cosmetics and care cosmetics.
Cosmetics that are meant to be used on the face and eye area are usually applied with a brush, a makeup sponge, or the fingertips.
Most cosmetics are distinguished by the area of the body intended for application.
The Types of Cosmetics follow:
- Primer comes in formulas to suit individual skin conditions. Most are meant to reduce the appearance of pore size, prolong the wear of makeup, and allow for a smoother application of makeup. Primers are applied before foundation.
- Lipstick, lip gloss, lip liner, lip plumper, lip balm, lip conditioner, lip primer, lip boosters, and lip butters: Lipsticks are intended to add color and texture to the lips and often come in a wide range of colors, as well as finishes such as matte, satin and lustre. Lip stains have a water or gel base and may contain alcohol to help the product stay on. They temporarily saturate the lips with a dye. Usually designed to be waterproof, the product may come with an applicator brush, rollerball, or be applied with a finger. Lip glosses are intended to add shine to the lips and may add a tint of color, as well as being scented or flavored. Lip balms are most often used to moisturize and protect the lips. They often contain SPF protection.
- Concealer makeup covers imperfections of the skin. Concealer is often used for any extra coverage needed to cover blemishes, under eye circles, and other imperfections. Concealer is often thicker and more solid than foundation, and provides longer lasting, more detailed coverage. Some formulations are meant only for the eye or only for the face. This product can also be used for contouring the face like ones nose, cheekbones, and jaw line.
- Foundation is used to smooth out the face and cover spots or uneven skin coloration. Usually a liquid, cream, or powder, as well as most recently a light and fluffy mousse. Foundation provides coverage from sheer to full. Foundation primer can be applied before or after foundation to obtain a smoother finish. Some primers come in powder or liquid form to be applied before foundation as a base, while other primers come as a spray to be applied after the foundation to help the make-up last longer.
- Face powder sets the foundation, giving it a matte finish, and to conceal small flaws or blemishes. Can also be used to bake the foundation, so it stays on longer. Tinted face powders may be worn alone as a light foundation.
- Rouge, blush or blusher is cheek coloring to bring out the color in the cheeks and make the cheekbones appear more defined. Rouge comes in powder, cream, and liquid forms.
- Contour powder/creams are used to define the face. They can give the illusion of a slimmer face or to modify a face shape in other desired ways. Usually a few shades darker than one's own skin tone and matte in finish, contour products create the illusion of depth. A darker toned foundation/concealer can be used instead of contour products for a more natural look.
- Highlight, used to draw attention to the high points of the face as well as to add glow, comes in liquid, cream, and powder forms. It often contains a substance to provide shimmer. A lighter toned foundation/concealer can be used instead of highlight to create a more natural look.
- Bronzer gives skin a bit of color by adding a golden or bronze glow and highlighting the cheekbones, as well as being used for contouring. Bronzer is considered to be more of a natural look and can be used for an everyday wear. Bronzer enhances the color of the face while adding more of a shimmery look. It comes in either matte, semi matte/satin, or shimmer finishes.
- Mascara is used to darken, lengthen, thicken, or draw attention to the eyelashes. It is available in natural colors such as brown and black, but also comes in bolder colors such as blue, pink, or purple. Some mascaras include glitter flecks. There are many formulas, including waterproof versions for those prone to allergies or sudden tears. It is often used after an eyelash curler and mascara primer. Many mascaras have components to help lashes appear longer and thicker.
- Eyeliner is used to enhance and elongate the size of the eye. For example, using white eyeliner on the waterline and inner corners of the eye helps to make the eyes look bigger and more awake.
- Eyebrow pencils, creams, waxes, gels and powders are color and define the brows.
- Nail polish is used to color the fingernails and toenails. Transparent, colorless versions may strengthen nails or as a top or base coat to protect the nail or polish.
- Setting spray is used as the last step in the process of applying makeup. It keeps applied makeup intact for long periods. An alternative to setting spray is setting powder, which may be either pigmented or translucent. Both of these products claim to keep makeup from absorbing into the skin or melting off.
- False eyelashes are frequently used when extravagant and exaggerated eyelashes are desired. Their basic design usually consists of human hair or synthetic materials attached to a thin cloth-like band, which is applied with an eyelash glue to the lash line. Designs vary from short, natural-looking lashes to extremely long, wispy, rainbow-colored lashes. Rhinestones, gems, and even feathers and lace occur on some false eyelash designs.
Cosmetics can be also described by the physical composition of the product. Cosmetics can be liquid or cream emulsions; powders, both pressed and loose; dispersions; and anhydrous creams or sticks.
Makeup remover is a product used to remove the makeup products applied on the skin. It cleans the skin before other procedures, like applying bedtime lotion.
Female Supermodels
YouTube Video: Elle Macpherson Walks Us Through a Typical Day in Her Life | E! Red Carpet & Live Events
Pictured: LEFT: Gisele Bündchen has been the world's highest-paid model since 2004; RIGHT: Christie Brinkley

A supermodel (also spelled super-model and super model) is a highly paid fashion model who usually has a worldwide reputation and often a background in haute couture and commercial modeling. The term supermodel became prominent in the popular culture of the 1980s.
Supermodels usually work for top fashion designers and famous clothing brands. They have multimillion-dollar contracts, endorsements and campaigns. They have branded themselves as household names and worldwide recognition is associated with their modeling careers.
They have been on the covers of prestigious magazines such as French, British, American, and Italian Vogue. Claudia Schiffer stated, "In order to become a supermodel one must be on all the covers all over the world at the same time so that people can recognize the girls."
Supermodels usually work for top fashion designers and famous clothing brands. They have multimillion-dollar contracts, endorsements and campaigns. They have branded themselves as household names and worldwide recognition is associated with their modeling careers.
They have been on the covers of prestigious magazines such as French, British, American, and Italian Vogue. Claudia Schiffer stated, "In order to become a supermodel one must be on all the covers all over the world at the same time so that people can recognize the girls."
Libido
YouTube Video Low Libido? Boost Your Sex Drive with These 10 Tips
Pictured: Top 10 most powerful foods for supporting male libido Aug. 21, 2015

Libido, colloquially known as sex drive, is a person's overall sexual drive or desire for sexual activity. Sex drive is influenced by biological, psychological and social factors.
Biologically, the sex hormones and associated neurotransmitters that act upon the nucleus accumbens (primarily testosterone and dopamine, respectively) regulate libido in men and women. Social factors, such as work and family, and internal psychological factors, like personality and stress, can affect libido.
Sex drive can also be affected by medical conditions, medications, lifestyle and relationship issues, and age (e.g., puberty). A person who has extremely frequent or a suddenly increased sex drive may be experiencing hypersexuality.
A person may have a desire for sex, but not have the opportunity to act on that desire, or may on personal, moral or religious reasons refrain from acting on the urge. Psychologically, a person's urge can be repressed or sublimated. On the other hand, a person can engage in sexual activity without an actual desire for it. Multiple factors affect human sex drive, including stress, illness, pregnancy, and others.
Sexual desires are often an important factor in the formation and maintenance of intimate relationships in both men and women. A lack or loss of sexual desire can adversely affect relationships. Changes in the sexual desires of either partner in a sexual relationship, if sustained and unresolved, may cause problems in the relationship.
The infidelity of a partner may be an indication that a partner's changing sexual desires can no longer be satisfied within the current relationship. Problems can arise from disparity of sexual desires between partners, or poor communication between partners of sexual needs and preferences.
A person is sex starved or sexually frustrated when they have a strong sexual appetite but is sexually frustrated because of a lack of outlet or companion to release their sexual tension.
Click on any of the following blue hyperlinks for further amplification:
Biologically, the sex hormones and associated neurotransmitters that act upon the nucleus accumbens (primarily testosterone and dopamine, respectively) regulate libido in men and women. Social factors, such as work and family, and internal psychological factors, like personality and stress, can affect libido.
Sex drive can also be affected by medical conditions, medications, lifestyle and relationship issues, and age (e.g., puberty). A person who has extremely frequent or a suddenly increased sex drive may be experiencing hypersexuality.
A person may have a desire for sex, but not have the opportunity to act on that desire, or may on personal, moral or religious reasons refrain from acting on the urge. Psychologically, a person's urge can be repressed or sublimated. On the other hand, a person can engage in sexual activity without an actual desire for it. Multiple factors affect human sex drive, including stress, illness, pregnancy, and others.
Sexual desires are often an important factor in the formation and maintenance of intimate relationships in both men and women. A lack or loss of sexual desire can adversely affect relationships. Changes in the sexual desires of either partner in a sexual relationship, if sustained and unresolved, may cause problems in the relationship.
The infidelity of a partner may be an indication that a partner's changing sexual desires can no longer be satisfied within the current relationship. Problems can arise from disparity of sexual desires between partners, or poor communication between partners of sexual needs and preferences.
A person is sex starved or sexually frustrated when they have a strong sexual appetite but is sexually frustrated because of a lack of outlet or companion to release their sexual tension.
Click on any of the following blue hyperlinks for further amplification:
- Psychological perspectives
- Psychoanalysis
- Analytical psychology
- Factors that affect libido
- Sexual desire disorders
- See also:
Marriage
YouTube Video: "Saying I Do: What Happens at a Catholic Wedding"
Pictured: Wedding ceremonies performed outdoor and indoor

Marriage, also called matrimony or wedlock, is a socially or ritually recognized union or legal contract between spouses that establishes rights and obligations between them, between them and their children, and between them and their in-laws, as well as society in general.
The definition of marriage varies according to different cultures, but it is principally an institution in which interpersonal relationships, usually sexual, are acknowledged. In some cultures, marriage is recommended or considered to be compulsory before pursuing any sexual activity. When defined broadly, marriage is considered a cultural universal.
Individuals may marry for several reasons, including legal, social, libidinal, emotional, financial, spiritual, and religious purposes. Whom they marry may be influenced by socially determined rules of incest, prescriptive marriage rules, parental choice and individual desire.
In some areas of the world, arranged marriage, child marriage, polygamy, and sometimes forced marriage, may be practiced as a cultural tradition.
Conversely, such practices may be outlawed and penalized in parts of the world out of concerns for women's rights and because of international law.
In developed parts of the world, there has been a general trend towards ensuring equal rights within marriage for women and legally recognizing the marriages of interfaith or interracial, and same-sex couples. These trends coincide with the broader human rights movement.
Marriage can be recognized by a state, an organization, a religious authority, a tribal group, a local community or peers. It is often viewed as a contract. Civil marriage, which does not exist in some countries, is marriage without religious content carried out by a government institution in accordance with the marriage laws of the jurisdiction, and recognized as creating the rights and obligations intrinsic to matrimony.
Marriages can be performed in a secular civil ceremony or in a religious setting via a wedding ceremony. The act of marriage usually creates normative or legal obligations between the individuals involved, and any offspring they may produce.
In terms of legal recognition, most sovereign states and other jurisdictions limit marriage to opposite-sex couples and a diminishing number of these permit polygyny, child marriages, and forced marriages.
Over the twentieth century, a growing number of countries and other jurisdictions have lifted bans on and have established legal recognition for interracial marriage, interfaith marriage, and most recently,same-sex marriage.
Some cultures allow the dissolution of marriage through divorce or annulment. In some areas, child marriages and polygamy may occur in spite of national laws against the practice.
Since the late twentieth century, major social changes in Western countries have led to changes in the demographics of marriage, with the age of first marriage increasing, fewer people marrying, and more couples choosing to cohabit rather than marry. For example, the number of marriages in Europe decreased by 30% from 1975 to 2005.
Historically, in most cultures, married women had very few rights of their own, being considered, along with the family's children, the property of the husband; as such, they could not own or inherit property, or represent themselves legally (see for example coverture).
In Europe, the United States, and other places in the developed world, beginning in the late 19th century and lasting through the 21st century, marriage has undergone gradual legal changes, aimed at improving the rights of the wife. These changes included giving wives legal identities of their own, abolishing the right of husbands to physically discipline their wives, giving wives property rights, liberalizing divorce laws, providing wives with reproductive rights of their own, and requiring a wife's consent when sexual relations occur. These changes have occurred primarily in Western countries.
In the 21st century, there continue to be controversies regarding the legal status of married women, legal acceptance of or leniency towards violence within marriage (especially sexual violence), traditional marriage customs such as dowry and bride price, forced marriage, marriageable age, and criminalization of consensual behaviors such as premarital and extramarital sex.
For additional amplification, click here.
The definition of marriage varies according to different cultures, but it is principally an institution in which interpersonal relationships, usually sexual, are acknowledged. In some cultures, marriage is recommended or considered to be compulsory before pursuing any sexual activity. When defined broadly, marriage is considered a cultural universal.
Individuals may marry for several reasons, including legal, social, libidinal, emotional, financial, spiritual, and religious purposes. Whom they marry may be influenced by socially determined rules of incest, prescriptive marriage rules, parental choice and individual desire.
In some areas of the world, arranged marriage, child marriage, polygamy, and sometimes forced marriage, may be practiced as a cultural tradition.
Conversely, such practices may be outlawed and penalized in parts of the world out of concerns for women's rights and because of international law.
In developed parts of the world, there has been a general trend towards ensuring equal rights within marriage for women and legally recognizing the marriages of interfaith or interracial, and same-sex couples. These trends coincide with the broader human rights movement.
Marriage can be recognized by a state, an organization, a religious authority, a tribal group, a local community or peers. It is often viewed as a contract. Civil marriage, which does not exist in some countries, is marriage without religious content carried out by a government institution in accordance with the marriage laws of the jurisdiction, and recognized as creating the rights and obligations intrinsic to matrimony.
Marriages can be performed in a secular civil ceremony or in a religious setting via a wedding ceremony. The act of marriage usually creates normative or legal obligations between the individuals involved, and any offspring they may produce.
In terms of legal recognition, most sovereign states and other jurisdictions limit marriage to opposite-sex couples and a diminishing number of these permit polygyny, child marriages, and forced marriages.
Over the twentieth century, a growing number of countries and other jurisdictions have lifted bans on and have established legal recognition for interracial marriage, interfaith marriage, and most recently,same-sex marriage.
Some cultures allow the dissolution of marriage through divorce or annulment. In some areas, child marriages and polygamy may occur in spite of national laws against the practice.
Since the late twentieth century, major social changes in Western countries have led to changes in the demographics of marriage, with the age of first marriage increasing, fewer people marrying, and more couples choosing to cohabit rather than marry. For example, the number of marriages in Europe decreased by 30% from 1975 to 2005.
Historically, in most cultures, married women had very few rights of their own, being considered, along with the family's children, the property of the husband; as such, they could not own or inherit property, or represent themselves legally (see for example coverture).
In Europe, the United States, and other places in the developed world, beginning in the late 19th century and lasting through the 21st century, marriage has undergone gradual legal changes, aimed at improving the rights of the wife. These changes included giving wives legal identities of their own, abolishing the right of husbands to physically discipline their wives, giving wives property rights, liberalizing divorce laws, providing wives with reproductive rights of their own, and requiring a wife's consent when sexual relations occur. These changes have occurred primarily in Western countries.
In the 21st century, there continue to be controversies regarding the legal status of married women, legal acceptance of or leniency towards violence within marriage (especially sexual violence), traditional marriage customs such as dowry and bride price, forced marriage, marriageable age, and criminalization of consensual behaviors such as premarital and extramarital sex.
For additional amplification, click here.
Pregnancy and Childbirth
YouTube Video: How to Support Partner during Labor | Pregnancy
YouTube Video: 9 Months In The Womb: A Remarkable Look At Fetal Development Through Ultrasound
Pregnancy, also known as gestation, is the time during which one or more offspring develops inside a woman.
A multiple pregnancy involves more than one offspring, such as with twins.
Pregnancy can occur by sexual intercourse or assisted reproductive technology.
Childbirth typically occurs around 40 weeks from the last menstrual period (LMP). This is just over nine months, where each month averages 29½ days.When measured from conception it is about 38 weeks.
An embryo is the developing offspring during the first eight weeks following conception, after which, the term fetus is used until birth.
Symptoms of early pregnancy may include missed periods, tender breasts, nausea and vomiting, hunger, and frequent urination. Pregnancy may be confirmed with a pregnancy test.
Pregnancy is typically divided into three trimesters. The first trimester is from week one through 12 and includes conception. Conception is when the sperm fertilizes the egg.
The fertilized egg then travels down the fallopian tube and attaches to the inside of the uterus, where it begins to form the embryo and placenta. The first trimester carries the highest risk of miscarriage (natural death of embryo or fetus). The second trimester is from week 13 through 28.
Around the middle of the second trimester, movement of the fetus may be felt. At 28 weeks, more than 90% of babies can survive outside of the uterus if provided with high-quality medical care. The third trimester is from 29 weeks through 40 weeks.
Prenatal care improves pregnancy outcomes. Prenatal care may include taking extra folic acid, avoiding drugs and alcohol, regular exercise, blood tests, and regular physical examinations.
Complications of pregnancy may include disorders of high blood pressure, gestational diabetes, iron-deficiency anemia, and severe nausea and vomiting among others.
Term pregnancy is 37 to 41 weeks, with early term being 37 and 38 weeks, full term 39 and 40 weeks, and late term 41 weeks.
After 41 weeks, it is known as post term. Babies born before 37 weeks are preterm and are at higher risk of health problems such as cerebral palsy. Delivery before 39 weeks by labor induction or caesarean section is not recommended unless required for other medical reasons.
About 213 million pregnancies occurred in 2012, of which, 190 million were in the developing world and 23 million were in the developed world. The number of pregnancies in women ages 15 to 44 is 133 per 1,000 women.
About 10% to 15% of recognized pregnancies end in miscarriage. In 2013, complications of pregnancy resulted in 293,000 deaths, down from 377,000 deaths in 1990. Common causes include maternal bleeding, complications of abortion, high blood pressure of pregnancy, maternal sepsis, and obstructed labor.
Globally, 40% of pregnancies are unplanned. Half of unplanned pregnancies are aborted. Among unintended pregnancies in the United States, 60% of the women used birth control to some extent during the month pregnancy occurred.
Click on any of the following blue hyperlinks for more about Pregnancy:
Childbirth, also known as labor and delivery, is the ending of a pregnancy by one or more babies leaving a woman's uterus by vaginal passage or C-section.
In 2015 there were about 135 million births globally. About 15 million were born before 37 weeks of gestation, while between 3 and 12% were born after 42 weeks.
In the developed world most deliveries occur in hospital, while in the developing world most births take place at home with the support of a traditional birth attendant.
The most common way of childbirth is a vaginal delivery. It involves three stages of labor:
The first stage typically lasts twelve to nineteen hours, the second stage twenty minutes to two hours, and the third stage five to thirty minutes.
The first stage begins with crampy abdominal or back pains that last around half a minute and occur every ten to thirty minutes. The crampy pains become stronger and closer together over time.
During the second stage pushing with contractions may occur.
In the third stage delayed clamping of the umbilical cord is generally recommended. A number of methods can help with pain such as relaxation techniques, opioids, and spinal blocks.
Most babies are born head first; however about 4% are born feet or buttock first, known as breech.
During labor a woman can generally eat and move around as she likes, but pushing is not recommended during the first stage or during delivery of the head, and enemas are not recommended.
While making a cut to the opening of the vagina is common, known as an episiotomy, it is generally not needed.
In 2012, about 23 million deliveries occurred by a surgical procedure known as Caesarean section. Caesarean sections may be recommended for twins, signs of distress in the baby, or breech position. This method of delivery can take longer to heal from.
Each year, complications from pregnancy and childbirth result in about 500,000 maternal deaths, 7 million women have serious long term problems, and 50 million women have health negative outcomes following delivery. Most of these occur in the developing world.
Specific complications include obstructed labor, postpartum bleeding, eclampsia, and postpartum infection. Complications in the baby include birth asphyxia.
Click on any of the following blue hyperlinks for more about Childbirth:
A multiple pregnancy involves more than one offspring, such as with twins.
Pregnancy can occur by sexual intercourse or assisted reproductive technology.
Childbirth typically occurs around 40 weeks from the last menstrual period (LMP). This is just over nine months, where each month averages 29½ days.When measured from conception it is about 38 weeks.
An embryo is the developing offspring during the first eight weeks following conception, after which, the term fetus is used until birth.
Symptoms of early pregnancy may include missed periods, tender breasts, nausea and vomiting, hunger, and frequent urination. Pregnancy may be confirmed with a pregnancy test.
Pregnancy is typically divided into three trimesters. The first trimester is from week one through 12 and includes conception. Conception is when the sperm fertilizes the egg.
The fertilized egg then travels down the fallopian tube and attaches to the inside of the uterus, where it begins to form the embryo and placenta. The first trimester carries the highest risk of miscarriage (natural death of embryo or fetus). The second trimester is from week 13 through 28.
Around the middle of the second trimester, movement of the fetus may be felt. At 28 weeks, more than 90% of babies can survive outside of the uterus if provided with high-quality medical care. The third trimester is from 29 weeks through 40 weeks.
Prenatal care improves pregnancy outcomes. Prenatal care may include taking extra folic acid, avoiding drugs and alcohol, regular exercise, blood tests, and regular physical examinations.
Complications of pregnancy may include disorders of high blood pressure, gestational diabetes, iron-deficiency anemia, and severe nausea and vomiting among others.
Term pregnancy is 37 to 41 weeks, with early term being 37 and 38 weeks, full term 39 and 40 weeks, and late term 41 weeks.
After 41 weeks, it is known as post term. Babies born before 37 weeks are preterm and are at higher risk of health problems such as cerebral palsy. Delivery before 39 weeks by labor induction or caesarean section is not recommended unless required for other medical reasons.
About 213 million pregnancies occurred in 2012, of which, 190 million were in the developing world and 23 million were in the developed world. The number of pregnancies in women ages 15 to 44 is 133 per 1,000 women.
About 10% to 15% of recognized pregnancies end in miscarriage. In 2013, complications of pregnancy resulted in 293,000 deaths, down from 377,000 deaths in 1990. Common causes include maternal bleeding, complications of abortion, high blood pressure of pregnancy, maternal sepsis, and obstructed labor.
Globally, 40% of pregnancies are unplanned. Half of unplanned pregnancies are aborted. Among unintended pregnancies in the United States, 60% of the women used birth control to some extent during the month pregnancy occurred.
Click on any of the following blue hyperlinks for more about Pregnancy:
- Terminology
- Signs and symptoms
- Chronology
- Physiology
- Diagnosis
- Management
- Complications
- Intercurrent diseases
- Medical imaging
- Epidemiology
- Society and culture
- See also:
- Pregnancy at DMOZ
- Merck Manual Home Health Handbook – further details on the diseases, disorders, etc., which may complicate pregnancy.
- Pregnancy care planner – NHS guide to having a baby including preconception, pregnancy, labor, and birth.
Childbirth, also known as labor and delivery, is the ending of a pregnancy by one or more babies leaving a woman's uterus by vaginal passage or C-section.
In 2015 there were about 135 million births globally. About 15 million were born before 37 weeks of gestation, while between 3 and 12% were born after 42 weeks.
In the developed world most deliveries occur in hospital, while in the developing world most births take place at home with the support of a traditional birth attendant.
The most common way of childbirth is a vaginal delivery. It involves three stages of labor:
- the shortening and opening of the cervix,
- descent and birth of the baby,
- and the delivery of the placenta.
The first stage typically lasts twelve to nineteen hours, the second stage twenty minutes to two hours, and the third stage five to thirty minutes.
The first stage begins with crampy abdominal or back pains that last around half a minute and occur every ten to thirty minutes. The crampy pains become stronger and closer together over time.
During the second stage pushing with contractions may occur.
In the third stage delayed clamping of the umbilical cord is generally recommended. A number of methods can help with pain such as relaxation techniques, opioids, and spinal blocks.
Most babies are born head first; however about 4% are born feet or buttock first, known as breech.
During labor a woman can generally eat and move around as she likes, but pushing is not recommended during the first stage or during delivery of the head, and enemas are not recommended.
While making a cut to the opening of the vagina is common, known as an episiotomy, it is generally not needed.
In 2012, about 23 million deliveries occurred by a surgical procedure known as Caesarean section. Caesarean sections may be recommended for twins, signs of distress in the baby, or breech position. This method of delivery can take longer to heal from.
Each year, complications from pregnancy and childbirth result in about 500,000 maternal deaths, 7 million women have serious long term problems, and 50 million women have health negative outcomes following delivery. Most of these occur in the developing world.
Specific complications include obstructed labor, postpartum bleeding, eclampsia, and postpartum infection. Complications in the baby include birth asphyxia.
Click on any of the following blue hyperlinks for more about Childbirth:
- Signs and symptoms
- Vaginal birth
- Onset of labour
First stage: latent phase
First stage: active phase
Second stage: fetal expulsion
Third stage: placenta delivery
Fourth stage
- Onset of labour
- Management
- Collecting stem cells
- Complications
- Society and culture
- See also:
- Advanced maternal age, when a woman is of an older age at reproduction
- Antinatalism
- Asynclitic birth, an abnormal birth position
- Bradley method of natural childbirth
- Coffin birth
- Kangaroo care
- Lamaze
- Obstetrical bleeding
- Naegele's Rule to calculate the due date for a pregnancy
- Natalism
- Natural childbirth
- Obstetrical Dilemma
- Pre- and perinatal psychology
- Reproductive Health Supplies Coalition
- Traditional birth attendant
- Unassisted childbirth
- Vernix caseosa
- Water birth
Romance
YouTube Video from the 1961 movie "Breakfast at Tiffany's"*,
Paul (George Peppard) says "I love you" to Holly Golightly (Audrey Hepburn) in Library Scene
*--Movie "Breakfast at Tiffany's"
Pictured: LEFT: Romeo and Juliet parting on the balcony in Act III; RIGHT: Poster of the 1970 Movie “The Love Story” Starring Ryan O’Neal and Ali MacGraw
Romance is the expressive and pleasurable feeling from an emotional attraction towards another person often associated with sexual attraction.
In the context of romantic love relationships, romance usually implies an expression of one's strong romantic love, or one's deep and strong emotional desires to connect with another person intimately or romantically. Historically, the term "romance" originates with the medieval ideal of chivalry as set out in its chivalric romance literature.
Humans have a natural inclination to form bonds with one another through social interactions, be it through verbal communication or nonverbal gestures.
Click in on any of the following blue hyperlinks for further amplification:
In the context of romantic love relationships, romance usually implies an expression of one's strong romantic love, or one's deep and strong emotional desires to connect with another person intimately or romantically. Historically, the term "romance" originates with the medieval ideal of chivalry as set out in its chivalric romance literature.
Humans have a natural inclination to form bonds with one another through social interactions, be it through verbal communication or nonverbal gestures.
Click in on any of the following blue hyperlinks for further amplification:
- General definitions
- Types
- In philosophy
- Tragedy and other social issues
- Psychology
- Helen Fisher
- John Townsend
- Karen Horney
- Harold Bessell
- Lisa M. Diamond
- Martie Haselton
- University research
- Major theories
- Attachment patterns
- Romantic love definition/operationalization
- Passionate and companionate love
- The triangular theory of love
- The self-expansion theory of romantic love
- Mindful relationships
- Relationship behaviors
- Applications
- Controversies
- See also:
- Platonic love
- Chivalric romance
- Romantic orientation
- Interpersonal attraction
- Courtly love
- Erotomania
- Erotophobia
- Infatuation
- Intimate relationship
- Love
- Marriage
- Love sickness
- Physical intimacy
- Romanticism
- Romantic friendship
- Romance novel
- Sexual relationship
- Valentine's Day
- The Four Loves
- True Romance
- Flirting
- Fraternizing
- Courtship
- Pet names
- Intimacy
- Interpersonal communication
- Romanticism
- Dating
Sex in Advertising
YouTube Video of Ellen's Reflections on Cialis and Viagra Commercials
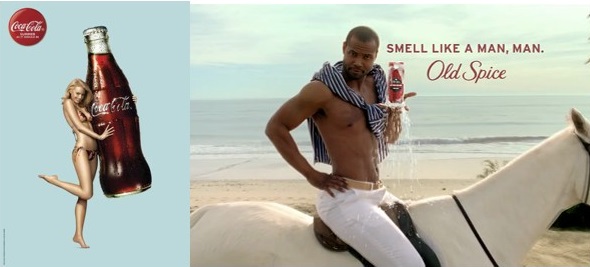
Sex in advertising or "sex sells" is the use of sex appeal in advertising to help sell a particular product or service. Sexually appealing imagery may or may not pertain to the product or service in question. Examples of sexually appealing imagery include nudity, pin-up girls, and muscular men.
The use of sex in advertising can be highly overt or extremely subtle. It ranges from relatively explicit displays of sexual acts and seductive behavior aimed at the viewer, to the use of basic cosmetics to enhance attractive features.
In the 21st century, the use of increasingly explicit sexual imagery in consumer-oriented print advertising has become almost commonplace. Ads for jeans, perfumes and many other products have featured provocative images that were designed to elicit sexual responses from as large a cross section of the population as possible, to shock by their ambivalence, or to appeal to repressed sexual desires, which are thought to carry a stronger emotional load.
Increased tolerance, more tempered censorship, emancipatory developments and increasing buying power of previously neglected appreciative target groups in rich markets (mainly in the West) have led to a marked increase in the share of attractive flesh 'on display'. Ad Age, a magazine delivering news, analysis, and data on marketing and media, published a list of Top 100 most effective advertising of the century, out of the 100, only 8 involved use of sex.
Unruly Media's viral video tracker lists the Top-20 most viewed car commercial viral videos. Only 1 uses sex, while the No.1 spot was held by VW's "The Force" ad. The overall top-spot (across all product segments), was held by VW's "Fun Theory" campaign, the most viewed viral video as of October 2011.
In international perspective, a 2008 comparison of nudity in television advertising in Brazil, Canada, China, Germany, South Korea, Thailand, and the United States reveals that China and the United States have the most demure ads, while Germany and Thailand exposed more of the female body. There is little variation in male undress.
See Also:
The use of sex in advertising can be highly overt or extremely subtle. It ranges from relatively explicit displays of sexual acts and seductive behavior aimed at the viewer, to the use of basic cosmetics to enhance attractive features.
In the 21st century, the use of increasingly explicit sexual imagery in consumer-oriented print advertising has become almost commonplace. Ads for jeans, perfumes and many other products have featured provocative images that were designed to elicit sexual responses from as large a cross section of the population as possible, to shock by their ambivalence, or to appeal to repressed sexual desires, which are thought to carry a stronger emotional load.
Increased tolerance, more tempered censorship, emancipatory developments and increasing buying power of previously neglected appreciative target groups in rich markets (mainly in the West) have led to a marked increase in the share of attractive flesh 'on display'. Ad Age, a magazine delivering news, analysis, and data on marketing and media, published a list of Top 100 most effective advertising of the century, out of the 100, only 8 involved use of sex.
Unruly Media's viral video tracker lists the Top-20 most viewed car commercial viral videos. Only 1 uses sex, while the No.1 spot was held by VW's "The Force" ad. The overall top-spot (across all product segments), was held by VW's "Fun Theory" campaign, the most viewed viral video as of October 2011.
In international perspective, a 2008 comparison of nudity in television advertising in Brazil, Canada, China, Germany, South Korea, Thailand, and the United States reveals that China and the United States have the most demure ads, while Germany and Thailand exposed more of the female body. There is little variation in male undress.
See Also:
- Gender advertisement
- Body image
- Promotional model
- Exploitation of women in mass media
- Family in advertising
- Killing Us Softly
- Miss Representation
- Sexual objectification
- Shock advertising
Victoria Secrets Fashions
YouTube Video The 2016 Victoria’s Secret Fashion Show Is Going To Paris!
Pictured: 2015 Victoria's Secret Angels include (left to right in each row) Adriana Lima, Alessandra Ambrosio, Behati Prinsloo, Candice Swanepoel,Taylor Marie Hill, Elsa Hosk and Jasmine Tookes (Martha Hunt, Stella Maxwell, Lais Ribeiro, Romee Strijd, Sara Sampaio, Lily Aldridge and Josephine Skriver not pictured)
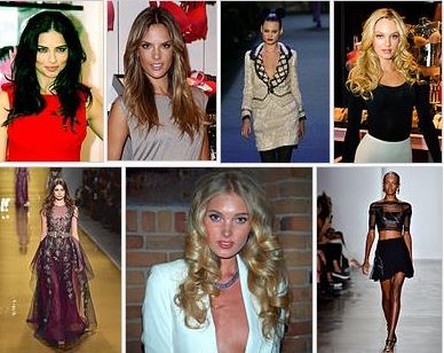
The Victoria's Secret Fashion Show is an annual fashion show sponsored by and featuring Victoria's Secret, a brand of lingerie and sleepwear. Victoria's Secret uses the show to promote and market its goods in high-profile settings.
The show features some of the world's leading fashion models such as current Victoria's Secret Angels Adriana Lima, Alessandra Ambrosio, Behati Prinsloo, Candice Swanepoel, and Lily Aldridge.
American network television broadcasts the show during prime time. The first few shows in the 1990s were held in the days preceding Valentine's Day to promote the brand for this holiday. They were not aired on national television. In 1999 and 2000 the show was webcast.
Beginning in 2001, the shows were moved ahead of the Christmas holiday season. Also in 2001, the show made its network television broadcast on ABC, though in all subsequent years, it has been broadcast on CBS.
The show has been held at a variety of locations in different cities including Miami, Los Angeles, and Cannes. The first four shows were held at the Plaza Hotel in New York City, but since it has become a televised event it has most often been held at the 69th Regiment Armory in New York City.
The show is a lavish event with elaborate costumed lingerie, varying music by leading entertainers, and set design according to the different themes running within the show. The show attracts hundreds of celebrities and entertainers, with special performers and acts every year.
Each year, twenty to forty of the world's top fashion models are selected to perform in the fashion show. In a typical year, this includes about a half dozen women under contract to the company, known as Victoria's Secret Angels, who help publicize the event. The giant angel wings worn by the models, as well as other wings of various forms and sizes such as butterfly, peacock, or devil wings, have become emblematic of the Victoria's Secret brand.
For additional Information, click here.
The show features some of the world's leading fashion models such as current Victoria's Secret Angels Adriana Lima, Alessandra Ambrosio, Behati Prinsloo, Candice Swanepoel, and Lily Aldridge.
American network television broadcasts the show during prime time. The first few shows in the 1990s were held in the days preceding Valentine's Day to promote the brand for this holiday. They were not aired on national television. In 1999 and 2000 the show was webcast.
Beginning in 2001, the shows were moved ahead of the Christmas holiday season. Also in 2001, the show made its network television broadcast on ABC, though in all subsequent years, it has been broadcast on CBS.
The show has been held at a variety of locations in different cities including Miami, Los Angeles, and Cannes. The first four shows were held at the Plaza Hotel in New York City, but since it has become a televised event it has most often been held at the 69th Regiment Armory in New York City.
The show is a lavish event with elaborate costumed lingerie, varying music by leading entertainers, and set design according to the different themes running within the show. The show attracts hundreds of celebrities and entertainers, with special performers and acts every year.
Each year, twenty to forty of the world's top fashion models are selected to perform in the fashion show. In a typical year, this includes about a half dozen women under contract to the company, known as Victoria's Secret Angels, who help publicize the event. The giant angel wings worn by the models, as well as other wings of various forms and sizes such as butterfly, peacock, or devil wings, have become emblematic of the Victoria's Secret brand.
For additional Information, click here.
Sex Symbols (Male and Female)
YouTube Video of Marilyn Monroe Singing Happy Birthday/Thanks For The Memories To President John F Kennedy 1962
Pictured: Posters of LEFT: Farrah Fawcett; RIGHT: Justin Bieber
A sex symbol is a celebrity of either sex, typically an actor, musician, supermodel, teen idol, or sports star, noted for being widely regarded as sexually attractive. The term was first used in the mid-1950s in relation to the popularity of certain film stars, including Marilyn Monroe, Brigitte Bardot, and Raquel Welch.
Click here for a Listing of Sex Symbols by Decade then Alphabetical.
Click here for a Listing of Sex Symbols by Decade then Alphabetical.
The Art of Seduction
YouTube Video from The Graduate (1967) - "Mrs. Robinson, you're trying to seduce me. Aren't you?"
Pictured: Dustin Hoffman and Anne Bancroft from "The Graduate" (1967)

Seduction is the process of deliberately enticing a person, to lead astray, as from duty, rectitude, or the like; to corrupt, to persuade or induce to engage in sexual behavior.
The word seduction stems from Latin and means literally "to lead astray". As a result, the term may have a positive or negative connotation.
Famous seducers from history or legend include Lilith, Giacomo Casanova and the fictional character Don Juan. Seduction as a phenomenon is not the subject of scientific interest, although similar, more specific terms like short-term mating, casual sex or mating strategies are used in evolutionary psychology.
The Internet enabled the existence of a seduction community which is based on pseudo-scientific discourse on seduction.
Seduction, seen negatively, involves temptation and enticement, often sexual in nature, to lead someone astray into a behavioral choice they would not have made if they were not in a state of sexual arousal.
Seen positively, seduction is a synonym for the act of charming someone — male or female — by an appeal to the senses, often with the goal of reducing unfounded fears and leading to their "sexual emancipation" Some sides in contemporary academic debate state that the morality of seduction depends on the long-term impacts on the individuals concerned, rather than the act itself, and may not necessarily carry the negative connotations expressed in dictionary definitions.
The word seduction stems from Latin and means literally "to lead astray". As a result, the term may have a positive or negative connotation.
Famous seducers from history or legend include Lilith, Giacomo Casanova and the fictional character Don Juan. Seduction as a phenomenon is not the subject of scientific interest, although similar, more specific terms like short-term mating, casual sex or mating strategies are used in evolutionary psychology.
The Internet enabled the existence of a seduction community which is based on pseudo-scientific discourse on seduction.
Seduction, seen negatively, involves temptation and enticement, often sexual in nature, to lead someone astray into a behavioral choice they would not have made if they were not in a state of sexual arousal.
Seen positively, seduction is a synonym for the act of charming someone — male or female — by an appeal to the senses, often with the goal of reducing unfounded fears and leading to their "sexual emancipation" Some sides in contemporary academic debate state that the morality of seduction depends on the long-term impacts on the individuals concerned, rather than the act itself, and may not necessarily carry the negative connotations expressed in dictionary definitions.
In Vitro Fertilization
YouTube Video: 3D animation of how IVF works
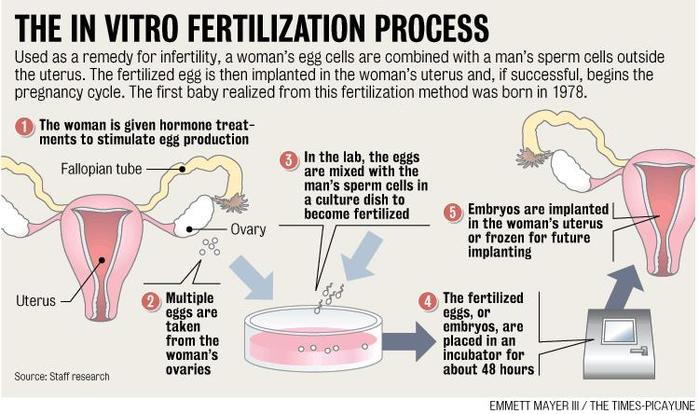
In vitro fertilization (or fertilization; IVF) is a process by which an egg is fertilized by sperm outside the body: in vitro ("in glass").
The process involves monitoring and stimulating a woman's ovulatory process, removing an ovum or ova (egg or eggs) from the woman's ovaries and letting sperm fertilize them in a liquid in a laboratory.
The fertilized egg (zygote) is cultured for 2–6 days in a growth medium and is then implanted in the same or another woman's uterus, with the intention of establishing a successful pregnancy.
IVF techniques can be used in different types of situations. It is a technique of assisted reproductive technology for treatment of infertility. IVF techniques are also employed in gestational surrogacy, in which case the fertilized egg is implanted into a surrogate's uterus, and the resulting child is genetically unrelated to the surrogate. In some situations, donated eggs or sperms may be used.
Some countries ban or otherwise regulate the availability of IVF treatment, giving rise to fertility tourism. Restrictions on availability of IVF include to single females, to lesbians and to surrogacy arrangements. Due to the costs of the procedure, IVF is mostly attempted only after less expensive options have failed.
The first successful birth of a "test tube baby", Louise Brown, occurred in 1978. Louise Brown was born as a result of natural cycle IVF where no stimulation was made.
Robert G. Edwards, the physiologist who developed the treatment, was awarded the Nobel Prize in Physiology or Medicine in 2010.
With egg donation and IVF, women who are past their reproductive years or menopause can still become pregnant. Adriana Iliescu held the record as the oldest woman to give birth using IVF and donated egg, when she gave birth in 2004 at the age of 66, a record passed in 2006.
After the IVF treatment many couples are able to get pregnant without any fertility treatments. In 2012 it was estimated that five million children had been born worldwide using IVF and other assisted reproduction techniques.
For further information (including availability and utilization), click here.
The process involves monitoring and stimulating a woman's ovulatory process, removing an ovum or ova (egg or eggs) from the woman's ovaries and letting sperm fertilize them in a liquid in a laboratory.
The fertilized egg (zygote) is cultured for 2–6 days in a growth medium and is then implanted in the same or another woman's uterus, with the intention of establishing a successful pregnancy.
IVF techniques can be used in different types of situations. It is a technique of assisted reproductive technology for treatment of infertility. IVF techniques are also employed in gestational surrogacy, in which case the fertilized egg is implanted into a surrogate's uterus, and the resulting child is genetically unrelated to the surrogate. In some situations, donated eggs or sperms may be used.
Some countries ban or otherwise regulate the availability of IVF treatment, giving rise to fertility tourism. Restrictions on availability of IVF include to single females, to lesbians and to surrogacy arrangements. Due to the costs of the procedure, IVF is mostly attempted only after less expensive options have failed.
The first successful birth of a "test tube baby", Louise Brown, occurred in 1978. Louise Brown was born as a result of natural cycle IVF where no stimulation was made.
Robert G. Edwards, the physiologist who developed the treatment, was awarded the Nobel Prize in Physiology or Medicine in 2010.
With egg donation and IVF, women who are past their reproductive years or menopause can still become pregnant. Adriana Iliescu held the record as the oldest woman to give birth using IVF and donated egg, when she gave birth in 2004 at the age of 66, a record passed in 2006.
After the IVF treatment many couples are able to get pregnant without any fertility treatments. In 2012 it was estimated that five million children had been born worldwide using IVF and other assisted reproduction techniques.
For further information (including availability and utilization), click here.
Surrogacy
YouTube Video: Traditional Surrogacy: How Does it Work?

A surrogacy arrangement or surrogacy agreement is the carrying of a pregnancy for intended parents.
There are two main types of surrogacy, gestational surrogacy (also known as host or full surrogacy) which was first achieved in April 1986 and traditional surrogacy (also known as partial, genetic, or straight surrogacy).
In gestational surrogacy, the pregnancy results from the transfer of an embryo created by in vitro fertilization (IVF), in a manner so the resulting child is genetically unrelated to the surrogate. Gestational surrogates are also referred to as gestational carriers.
In traditional surrogacy, the surrogate is impregnated naturally or artificially, but the resulting child is genetically related to the surrogate. In the United States, gestational surrogacy is more common than traditional surrogacy and is considered less legally complex.
Intended parents may seek a surrogacy arrangement when either pregnancy is medically impossible, pregnancy risks present an unacceptable danger to the mother's health or is a same sex couple's preferred method of procreation.
Monetary compensation may or may not be involved in these arrangements. If the surrogate receives money for the surrogacy the arrangement is considered commercial surrogacy, if she receives no compensation beyond reimbursement of medical and other reasonable expenses it is referred to as altruistic. The legality and costs of surrogacy vary widely between jurisdictions, sometimes resulting in interstate or international surrogacy arrangements.
Click on any of the following for amplification:
There are two main types of surrogacy, gestational surrogacy (also known as host or full surrogacy) which was first achieved in April 1986 and traditional surrogacy (also known as partial, genetic, or straight surrogacy).
In gestational surrogacy, the pregnancy results from the transfer of an embryo created by in vitro fertilization (IVF), in a manner so the resulting child is genetically unrelated to the surrogate. Gestational surrogates are also referred to as gestational carriers.
In traditional surrogacy, the surrogate is impregnated naturally or artificially, but the resulting child is genetically related to the surrogate. In the United States, gestational surrogacy is more common than traditional surrogacy and is considered less legally complex.
Intended parents may seek a surrogacy arrangement when either pregnancy is medically impossible, pregnancy risks present an unacceptable danger to the mother's health or is a same sex couple's preferred method of procreation.
Monetary compensation may or may not be involved in these arrangements. If the surrogate receives money for the surrogacy the arrangement is considered commercial surrogacy, if she receives no compensation beyond reimbursement of medical and other reasonable expenses it is referred to as altruistic. The legality and costs of surrogacy vary widely between jurisdictions, sometimes resulting in interstate or international surrogacy arrangements.
Click on any of the following for amplification:
- Types of surrogacy
- Gestational surrogacy (GS)
- Gestational surrogacy with embryo from both intended parents (GS/IP)
- Gestational surrogacy and egg donation (GS/ED)
- Gestational surrogacy and donor sperm (GS/DS)
- Gestational surrogacy and donor embryo (GS/DE)
- Traditional surrogacy (TS)
- Traditional surrogacy and donor sperm (TS/DS)
- Surrogacy centers
- Legal issues
- Surrogacy laws: United States
- Ethical issues
- Religious issues:
- Psychological concerns:
- See also:
Transgender
YouTube Video: Transgender swimmer now on Harvard men's team
Pictured: Before the After transgender reversal operation.
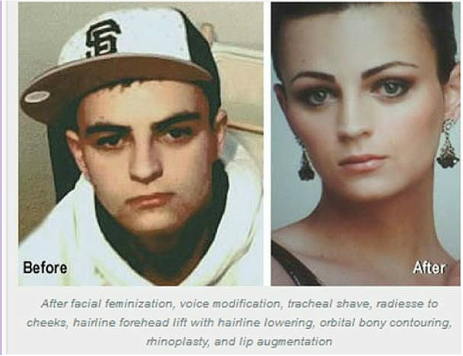
Transgender people experience a mismatch between their gender identity or gender expression and their assigned sex.
Transgender is also an umbrella term because, in addition to including trans men and trans women whose binary gender identity is the opposite of their assigned sex (and who are sometimes specifically termed transsexual if they desire medical assistance to transition), it may include gender queer people (whose identities are not exclusively masculine or feminine, but may, for example, be bigender, pangender, genderfluid, or agender).
Other definitions include third-gender people as transgender or conceptualize transgender people as a third gender, and infrequently the term is defined very broadly to include cross-dressers.
Many transgender people experience a period of identity development. The degree to which individuals feel genuine, authentic, and comfortable within their external appearance and accept their genuine identity is referred to as transgender congruence.
Being transgender is independent of sexual orientation; transgender people may identify as heterosexual, homosexual, bisexual, asexual, etc., or may consider conventional sexual orientation labels inadequate or inapplicable.
One effort to quantify the population gave a "rough estimate" that 0.3 percent of adults in the U.S. (1-in-300) are transgender, overlapping to an unknown degree with the estimated 3.5 percent of US adults (1-in-30) who identify as LGB.
Click here for further amplification.
Transgender is also an umbrella term because, in addition to including trans men and trans women whose binary gender identity is the opposite of their assigned sex (and who are sometimes specifically termed transsexual if they desire medical assistance to transition), it may include gender queer people (whose identities are not exclusively masculine or feminine, but may, for example, be bigender, pangender, genderfluid, or agender).
Other definitions include third-gender people as transgender or conceptualize transgender people as a third gender, and infrequently the term is defined very broadly to include cross-dressers.
Many transgender people experience a period of identity development. The degree to which individuals feel genuine, authentic, and comfortable within their external appearance and accept their genuine identity is referred to as transgender congruence.
Being transgender is independent of sexual orientation; transgender people may identify as heterosexual, homosexual, bisexual, asexual, etc., or may consider conventional sexual orientation labels inadequate or inapplicable.
One effort to quantify the population gave a "rough estimate" that 0.3 percent of adults in the U.S. (1-in-300) are transgender, overlapping to an unknown degree with the estimated 3.5 percent of US adults (1-in-30) who identify as LGB.
Click here for further amplification.
Sex Reassignment Surgery: Male to Female
YouTube Video: Caitlyn Jenner: Facial Feminization + Poses On Vanity Fair Cover | Good Morning America | ABC News
Pictured: Before we were introduced to Caitlyn Jenner, Bruce Jenner captured the hearts of America exactly 39 years ago Thursday by winning the gold medal in the men's decathlon at the 1976 Summer Olympics in Montreal.
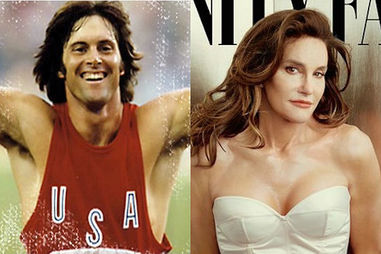
Sex reassignment surgery for male-to-female
involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures.
For genital surgery techniques click on: Vaginoplasty
Surgeon's requirements, procedures, and recommendations vary enormously in the days before and after, and the months following, these procedures.
Plastic surgery:
Since plastic surgery involves skin, is never an exact procedure, and cosmetic refining to the outer vulva is sometimes required. Some surgeons prefer to do most of the crafting of the outer vulva as a second surgery, when other tissues, blood and nerve supplies have recovered from the first surgery. This relatively minor surgery, which is usually performed only under local anaesthetic, is called labiaplasty.
The aesthetic, sensational, and functional results of vaginoplasty vary greatly. Surgeons vary considerably in their techniques and skills, patients' skin varies in elasticity and healing ability (which is affected by age, nutrition, physical activity and smoking), any previous surgery in the area can impact results, and surgery can be complicated by problems such as infections, blood loss, or nerve damage.
Supporters of colovaginoplasty state that this method is better than use of skin grafts for the reason that colon is already mucosal, whereas skin is not. However, many post-op trans women report that the skin used to line their vaginas develops mucosal qualities from months to years post-op.
For others, lubrication is needed when having sex and occasional douching is advised so that bacteria does not start to grow and give off odors.
Because the human body treats the new vagina as a wound, any current technique of vaginoplasty requires some long-term maintenance of volume (vaginal dilation), by the patient, using medical graduated dilators, dildos, or suitable substitutes, to keep the vagina open. Sexual intercourse is not an adequate method of performing dilation.
Regular application of estrogen into the vagina, for which there are several standard products, may help, but this must be calculated into total estrogen dose. Some surgeons have techniques to ensure continued depth, but extended periods without dilation will still often result in reduced diameter (vaginal stenosis) to some degree, which would require stretching again, either gradually, or, in extreme cases, under anaesthetic.
With current procedures, trans women do not have ovaries or uteri. This means that they are unable to bear children or menstruate until a uterus transplant is performed, and that they will need to remain on hormone therapy after their surgery to maintain female hormonal status.
Facial feminization surgery:
Occasionally these basic procedures are complemented further with feminizing cosmetic surgeries or procedures that modify bone or cartilage structures, typically in the jaw, brow, forehead, nose and cheek areas. These are known as facial feminization surgery or FFS.
Breast augmentation:
is the enlargement of the breasts. Some trans women choose to undergo this procedure if hormone therapy does not yield satisfactory results. Usually, typical growth for trans women is one to two cup sizes below closely related females such as the mother or sisters. Estrogen is responsible for fat distribution to the breasts, hips and buttocks, while progesterone is responsible for developing the actual milk glands. Progesterone also rounds out the breast to an adult tanner stage 5 shape and matures and darkens the areola.
Voice feminization surgery:
See also: Voice therapy (trans) and Vocal surgeries:
Because estrogens by themselves are not able to alter a person's voice range or pitch, some people proceed to seek treatment. Other options are available to people wishing to speak in a less masculine tone. Voice feminization lessons are available to train trans women to practice feminization of their speech.
Tracheal shave: is also sometimes used to reduce the cartilage in the area of the throat to conform to more feminine dimensions, to greatly reduce the appearance of an Adam's apple.
Buttock augmentation: because anatomically masculine hips and buttocks are generally smaller than those that are anatomically feminine, some MTF individuals will choose to undergo . If, however, efficient hormone therapy is conducted before the patient is past puberty, the pelvis will broaden slightly, and even if the patient is past their teen years, a layer of subcutaneous fat will be distributed over the body rounding contours.
Trans women usually end up with a waist to hip ratio of around 0.8, and if estrogen is administered at a young enough age "before the bone plates close", some trans women may achieve a waist to hip ratio of 0.7 or lower. The pubescent pelvis will broaden under estrogen therapy even if the skeleton is anatomically masculine.
Click here for further amplification.
involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures.
For genital surgery techniques click on: Vaginoplasty
Surgeon's requirements, procedures, and recommendations vary enormously in the days before and after, and the months following, these procedures.
Plastic surgery:
Since plastic surgery involves skin, is never an exact procedure, and cosmetic refining to the outer vulva is sometimes required. Some surgeons prefer to do most of the crafting of the outer vulva as a second surgery, when other tissues, blood and nerve supplies have recovered from the first surgery. This relatively minor surgery, which is usually performed only under local anaesthetic, is called labiaplasty.
The aesthetic, sensational, and functional results of vaginoplasty vary greatly. Surgeons vary considerably in their techniques and skills, patients' skin varies in elasticity and healing ability (which is affected by age, nutrition, physical activity and smoking), any previous surgery in the area can impact results, and surgery can be complicated by problems such as infections, blood loss, or nerve damage.
Supporters of colovaginoplasty state that this method is better than use of skin grafts for the reason that colon is already mucosal, whereas skin is not. However, many post-op trans women report that the skin used to line their vaginas develops mucosal qualities from months to years post-op.
For others, lubrication is needed when having sex and occasional douching is advised so that bacteria does not start to grow and give off odors.
Because the human body treats the new vagina as a wound, any current technique of vaginoplasty requires some long-term maintenance of volume (vaginal dilation), by the patient, using medical graduated dilators, dildos, or suitable substitutes, to keep the vagina open. Sexual intercourse is not an adequate method of performing dilation.
Regular application of estrogen into the vagina, for which there are several standard products, may help, but this must be calculated into total estrogen dose. Some surgeons have techniques to ensure continued depth, but extended periods without dilation will still often result in reduced diameter (vaginal stenosis) to some degree, which would require stretching again, either gradually, or, in extreme cases, under anaesthetic.
With current procedures, trans women do not have ovaries or uteri. This means that they are unable to bear children or menstruate until a uterus transplant is performed, and that they will need to remain on hormone therapy after their surgery to maintain female hormonal status.
Facial feminization surgery:
Occasionally these basic procedures are complemented further with feminizing cosmetic surgeries or procedures that modify bone or cartilage structures, typically in the jaw, brow, forehead, nose and cheek areas. These are known as facial feminization surgery or FFS.
Breast augmentation:
is the enlargement of the breasts. Some trans women choose to undergo this procedure if hormone therapy does not yield satisfactory results. Usually, typical growth for trans women is one to two cup sizes below closely related females such as the mother or sisters. Estrogen is responsible for fat distribution to the breasts, hips and buttocks, while progesterone is responsible for developing the actual milk glands. Progesterone also rounds out the breast to an adult tanner stage 5 shape and matures and darkens the areola.
Voice feminization surgery:
See also: Voice therapy (trans) and Vocal surgeries:
Because estrogens by themselves are not able to alter a person's voice range or pitch, some people proceed to seek treatment. Other options are available to people wishing to speak in a less masculine tone. Voice feminization lessons are available to train trans women to practice feminization of their speech.
Tracheal shave: is also sometimes used to reduce the cartilage in the area of the throat to conform to more feminine dimensions, to greatly reduce the appearance of an Adam's apple.
Buttock augmentation: because anatomically masculine hips and buttocks are generally smaller than those that are anatomically feminine, some MTF individuals will choose to undergo . If, however, efficient hormone therapy is conducted before the patient is past puberty, the pelvis will broaden slightly, and even if the patient is past their teen years, a layer of subcutaneous fat will be distributed over the body rounding contours.
Trans women usually end up with a waist to hip ratio of around 0.8, and if estrogen is administered at a young enough age "before the bone plates close", some trans women may achieve a waist to hip ratio of 0.7 or lower. The pubescent pelvis will broaden under estrogen therapy even if the skeleton is anatomically masculine.
Click here for further amplification.
Sex Reassignment Surgery: Female to Male
YouTube Video of Schuyler Bailar appearing on the Ellen Show about his Transgender surgery
Pictured: Featured on 60 Minutes April 10, 2016 segment interviewed by Leslie Stahl: Schuyler Bailar, Harvard Student who underwent female-to-male Sex Reassignment Surgery

Sex reassignment surgery from female to male includes a variety of surgical procedures for transgender men that alter female anatomical traits to provide physical traits more appropriate to the trans man's male identity and functioning.
Many trans men considering the option do not opt for genital reassignment surgery; more frequent surgical options include bilateral mastectomy (removal of the breasts) and chest contouring (providing a more typically male chest shape), and hysterectomy (the removal of internal sex organs).
Sex reassignment surgery is usually preceded by beginning hormone treatment with testosterone.
Masectomy:
Many trans men seek bilateral mastectomy, also called "top surgery", the removal of the breasts and the shaping of a male contoured chest.
Trans men with moderate to large breasts usually require a formal bilateral mastectomy with grafting and reconstruction of the nipple-areola. This will result in two horizontal scars on the lower edge of the pectoralis muscle, but allows for easier resizing of the nipple and placement in a typically male position.
By some doctors, the surgery is done in two steps, first the contents of the breast are removed through either a cut inside the areola or around it, and then let the skin retract for about a year, where in a second surgery the excess skin is removed.
This technique results in far less scarring, and the nipple-areola doesn't need to be removed and grafted. Completely removing and grafting often results in a loss of sensation of that area that may take months to over a year to return, or may never return at all; and in rare cases in the complete loss of this tissue.
In these rare cases, a nipple can be reconstructed as it is for surgical candidates whose nipples are removed as part of treatment for breast cancer.
For trans men with smaller breasts, a peri-areolar or "keyhole" procedure may be done where the mastectomy is performed through an incision made around the areola. This avoids the larger scars of a traditional mastectomy, but the nipples may be larger and may not be in a perfectly male orientation on the chest wall. In addition, there is less denervation (damage to the nerves supplying the skin) of the chest wall with a peri-areolar mastectomy, and less time is required for sensation to return. See Male Chest Reconstruction.
Hysterectomy
is the removal of the uterus. Bilateral salpingo-oophorectomy (BSO) is the removal of both ovaries and fallopian tubes. Hysterectomy without BSO in women is sometimes erroneously referred to as a 'partial hysterectomy' and is done to treat uterine disease while maintaining the female hormonal milieu until natural menopause occurs. A 'partial hysterectomy' is actually when the uterus is removed, but the cervix is left intact. If the cervix is removed, it is called a 'total hysterectomy.'
Some trans men desire to have a hysterectomy/BSO because of a discomfort with having internal female reproductive organs despite the fact that menses usually cease with hormonal therapy. Some undergo this as their only gender-identity confirming 'bottom surgery'. In other cases, sterilization may be required by the state in order for the sex marker on official documents to be changed.
For many trans men however, hysterectomy/BSO is done to decrease the risk of developing cervical, endometrial, and ovarian cancer. (Though like breast cancer, the risk does not become zero, but is drastically decreased.) It is unknown whether the risk of ovarian cancer is increased, decreased, or unchanged in transgender men.
The risk will probably never be known since the overall population of transgender men is very small; even within the population of transgender men on hormone therapy, many patients are at significantly decreased risk due to prior oophorectomy (removal of the ovaries).
While the rates of endometrial and cervical cancer are overall higher than ovarian cancer, and these malignancies occur in younger people, it is still highly unlikely that this question will ever be definitively answered.
Decreasing cancer risk is however, particularly important as trans men often feel uncomfortable seeking gynecologic care, and many do not have access to adequate and culturally sensitive treatment. Though ideally, even after hysterectomy/BSO, trans men should see a gynecologist for a check-up at least every three years. This is particularly the case for trans men who:
One important consideration is that any trans man who develops vaginal bleeding after successfully ceasing menses on testosterone, must be evaluated by a gynecologist. This is equivalent to post-menopausal bleeding in a woman and may herald the development of a gynecologic cancer.
Genital reconstructive procedures (GRT)
Use either the clitoris, which is enlarged by androgenic hormones (Metoidioplasty), or rely on free tissue grafts from the arm, the thigh or belly and an erectile prosthetic (Phalloplasty).
In either case, the urethra can be rerouted through the phallus to allow urination through the newly constructed penis. The labia majora are united to form a scrotum, where prosthetic testicles can be inserted.
Many trans men considering the option do not opt for genital reassignment surgery; more frequent surgical options include bilateral mastectomy (removal of the breasts) and chest contouring (providing a more typically male chest shape), and hysterectomy (the removal of internal sex organs).
Sex reassignment surgery is usually preceded by beginning hormone treatment with testosterone.
Masectomy:
Many trans men seek bilateral mastectomy, also called "top surgery", the removal of the breasts and the shaping of a male contoured chest.
Trans men with moderate to large breasts usually require a formal bilateral mastectomy with grafting and reconstruction of the nipple-areola. This will result in two horizontal scars on the lower edge of the pectoralis muscle, but allows for easier resizing of the nipple and placement in a typically male position.
By some doctors, the surgery is done in two steps, first the contents of the breast are removed through either a cut inside the areola or around it, and then let the skin retract for about a year, where in a second surgery the excess skin is removed.
This technique results in far less scarring, and the nipple-areola doesn't need to be removed and grafted. Completely removing and grafting often results in a loss of sensation of that area that may take months to over a year to return, or may never return at all; and in rare cases in the complete loss of this tissue.
In these rare cases, a nipple can be reconstructed as it is for surgical candidates whose nipples are removed as part of treatment for breast cancer.
For trans men with smaller breasts, a peri-areolar or "keyhole" procedure may be done where the mastectomy is performed through an incision made around the areola. This avoids the larger scars of a traditional mastectomy, but the nipples may be larger and may not be in a perfectly male orientation on the chest wall. In addition, there is less denervation (damage to the nerves supplying the skin) of the chest wall with a peri-areolar mastectomy, and less time is required for sensation to return. See Male Chest Reconstruction.
Hysterectomy
is the removal of the uterus. Bilateral salpingo-oophorectomy (BSO) is the removal of both ovaries and fallopian tubes. Hysterectomy without BSO in women is sometimes erroneously referred to as a 'partial hysterectomy' and is done to treat uterine disease while maintaining the female hormonal milieu until natural menopause occurs. A 'partial hysterectomy' is actually when the uterus is removed, but the cervix is left intact. If the cervix is removed, it is called a 'total hysterectomy.'
Some trans men desire to have a hysterectomy/BSO because of a discomfort with having internal female reproductive organs despite the fact that menses usually cease with hormonal therapy. Some undergo this as their only gender-identity confirming 'bottom surgery'. In other cases, sterilization may be required by the state in order for the sex marker on official documents to be changed.
For many trans men however, hysterectomy/BSO is done to decrease the risk of developing cervical, endometrial, and ovarian cancer. (Though like breast cancer, the risk does not become zero, but is drastically decreased.) It is unknown whether the risk of ovarian cancer is increased, decreased, or unchanged in transgender men.
The risk will probably never be known since the overall population of transgender men is very small; even within the population of transgender men on hormone therapy, many patients are at significantly decreased risk due to prior oophorectomy (removal of the ovaries).
While the rates of endometrial and cervical cancer are overall higher than ovarian cancer, and these malignancies occur in younger people, it is still highly unlikely that this question will ever be definitively answered.
Decreasing cancer risk is however, particularly important as trans men often feel uncomfortable seeking gynecologic care, and many do not have access to adequate and culturally sensitive treatment. Though ideally, even after hysterectomy/BSO, trans men should see a gynecologist for a check-up at least every three years. This is particularly the case for trans men who:
- retain their vagina (whether before or after further genital reconstruction,)
- have a strong family history or cancers of the breast, ovary, or uterus (endometrium,)
- have a personal history of gynecological cancer or significant dysplasia on a Pap smear.
One important consideration is that any trans man who develops vaginal bleeding after successfully ceasing menses on testosterone, must be evaluated by a gynecologist. This is equivalent to post-menopausal bleeding in a woman and may herald the development of a gynecologic cancer.
Genital reconstructive procedures (GRT)
Use either the clitoris, which is enlarged by androgenic hormones (Metoidioplasty), or rely on free tissue grafts from the arm, the thigh or belly and an erectile prosthetic (Phalloplasty).
In either case, the urethra can be rerouted through the phallus to allow urination through the newly constructed penis. The labia majora are united to form a scrotum, where prosthetic testicles can be inserted.
Lesbians, Gays, Bisexuals, and Transgenders ("LGBT")
YouTube Video: Secretary of State Hillary Clinton's Historic LGBT Speech
Pictured: LGBT publications, pride parades, and related events, such as this stage at Bologna Pride 2008 in Italy, increasingly drop the LGBT initialism instead of regularly adding new letters, and dealing with issues of placement of those letters within the new title.

LGBT or GLBT is an acronym that stands for lesbian, gay, bisexual, and transgender.
In use since the 1990s, the term is an adaptation of the initialism LGB, which was used to replace the term gay in reference to the LGBT community beginning in the mid-to-late 1980s. Activists believed that the term gay community did not accurately represent all those to whom it referred.
LGBT has become mainstream as a self-designation; it has been adopted by the majority of sexuality and gender identity-based community centers and media in the United States, as well as some other English-speaking countries. The term is used also in some other countries, particularly those which languages use the initialism, such as Argentina, France and Turkey.
The initialism LGBT is intended to emphasize a diversity of sexuality and gender identity-based cultures. It may be used to refer to anyone who is non-heterosexual or non-cisgender, instead of exclusively to people who are lesbian, gay, bisexual, or transgender.
To recognize this inclusion, a popular variant adds the letter Q for those who identify as queer or are questioning their sexual identity; LGBTQ has been recorded since 1996.
Those who wish to include intersex people in LGBT groups suggest an extended initialism LGBTI. LGBT is used in all parts of "The Activist's Guide" of the Yogyakarta Principles in Action. Some people combine the two acronyms and use the term LGBTIQ.
Whether or not LGBT people openly identify themselves may depend on local political concerns and whether they live in a discriminatory environment, as well as on the status of LGBT rights where they live.
In use since the 1990s, the term is an adaptation of the initialism LGB, which was used to replace the term gay in reference to the LGBT community beginning in the mid-to-late 1980s. Activists believed that the term gay community did not accurately represent all those to whom it referred.
LGBT has become mainstream as a self-designation; it has been adopted by the majority of sexuality and gender identity-based community centers and media in the United States, as well as some other English-speaking countries. The term is used also in some other countries, particularly those which languages use the initialism, such as Argentina, France and Turkey.
The initialism LGBT is intended to emphasize a diversity of sexuality and gender identity-based cultures. It may be used to refer to anyone who is non-heterosexual or non-cisgender, instead of exclusively to people who are lesbian, gay, bisexual, or transgender.
To recognize this inclusion, a popular variant adds the letter Q for those who identify as queer or are questioning their sexual identity; LGBTQ has been recorded since 1996.
Those who wish to include intersex people in LGBT groups suggest an extended initialism LGBTI. LGBT is used in all parts of "The Activist's Guide" of the Yogyakarta Principles in Action. Some people combine the two acronyms and use the term LGBTIQ.
Whether or not LGBT people openly identify themselves may depend on local political concerns and whether they live in a discriminatory environment, as well as on the status of LGBT rights where they live.
Sex Education in the United States
YouTube Video RE: Funny Take on Sex Education: Last Week Tonight with John Oliver (HBO)
Sex education in the United States is taught in two main forms: Comprehensive Sex Education and abstinence-only:
Most adolescents in the United States receive some form of sex education at school at least once between grades 6 and 12; many schools begin addressing some topics as early as grades 4 or 5. Academic and other proponents of the National Sexuality Education Standards advocate that by the end of the fifth grade, students should be able to "Define sexual orientation as the romantic attraction of an individual to someone of the same gender or a different gender."
However, what students learn varies widely, because curriculum decisions are so decentralized. Many states have laws governing what is taught in sex education classes or allowing parents to opt out. Some state laws leave curriculum decisions to individual school districts.
National public health goals for adolescents recommend providing a comprehensive sex education, which covers a wide array of topics and call for "increasing the share of adolescents receiving formal instruction about abstinence, birth control methods, and prevention of HIV/AIDS and STIs."
Despite the aims national public health goals, research has indicated a growing gap between them and adolescents receipt of sex education. Data from the National Survey of Family Growth, a nationally-representative household survey conducted by the National Center for Health Statistics, asked respondents if prior to age 18 they had ever received "any formal instruction at a school, church, a community center or some other place" about a range of sex education topics.
During the period 2011-2013, data from the NSFG showed that among adolescents aged 15–19, similar proportions of females and males reported receiving formal instruction, with the share receiving instruction about birth control methods (60% females, 55% males) lower than the share receiving instruction about saying no to sex, sexually transmitted diseases, or HIV/AIDS.
Many sexually experienced teens (43% females and 57% of females) do not receive formal instruction about contraception before they first have sex; the share of adolescents receiving formal instruction has been declining.
Between 2006-2010 and 2011-2013, there were declines in the proportion of females ages 15–19 who reported receiving instruction on birth control, saying no to sex, HIV/AIDS and sexually transmitted diseases, as well as a decline in the proportion of males who reported receiving formal instruction about birth control.
Both males and females reported an increase in receiving instruction on saying no to sex, without being provided information about birth control.
The NSFG also documents large declines in formal instruction about birth control from 1995 to 2011-2013 falling from 87% to 60% of adolescent females and 81% to 55% of adolescent males.
Although formal instruction on birth control has significantly declined, 9 out of 10 adolescents report receiving formal instruction about STDs.
Click here for additional information about Sex Education in the United States.
- Comprehensive sex education covers abstinence as a choice option, but also informs adolescents about human sexuality, age of consent and the availability of contraception and techniques to avoid contraction of sexually transmitted diseases.
- Abstinence-only sex education emphasizes abstinence from sexual activity prior to marriage and rejects methods such as contraception. The difference between the two approaches, and their impact on the behavior of adolescents, remains a controversial subject in the United States.
Most adolescents in the United States receive some form of sex education at school at least once between grades 6 and 12; many schools begin addressing some topics as early as grades 4 or 5. Academic and other proponents of the National Sexuality Education Standards advocate that by the end of the fifth grade, students should be able to "Define sexual orientation as the romantic attraction of an individual to someone of the same gender or a different gender."
However, what students learn varies widely, because curriculum decisions are so decentralized. Many states have laws governing what is taught in sex education classes or allowing parents to opt out. Some state laws leave curriculum decisions to individual school districts.
National public health goals for adolescents recommend providing a comprehensive sex education, which covers a wide array of topics and call for "increasing the share of adolescents receiving formal instruction about abstinence, birth control methods, and prevention of HIV/AIDS and STIs."
Despite the aims national public health goals, research has indicated a growing gap between them and adolescents receipt of sex education. Data from the National Survey of Family Growth, a nationally-representative household survey conducted by the National Center for Health Statistics, asked respondents if prior to age 18 they had ever received "any formal instruction at a school, church, a community center or some other place" about a range of sex education topics.
During the period 2011-2013, data from the NSFG showed that among adolescents aged 15–19, similar proportions of females and males reported receiving formal instruction, with the share receiving instruction about birth control methods (60% females, 55% males) lower than the share receiving instruction about saying no to sex, sexually transmitted diseases, or HIV/AIDS.
Many sexually experienced teens (43% females and 57% of females) do not receive formal instruction about contraception before they first have sex; the share of adolescents receiving formal instruction has been declining.
Between 2006-2010 and 2011-2013, there were declines in the proportion of females ages 15–19 who reported receiving instruction on birth control, saying no to sex, HIV/AIDS and sexually transmitted diseases, as well as a decline in the proportion of males who reported receiving formal instruction about birth control.
Both males and females reported an increase in receiving instruction on saying no to sex, without being provided information about birth control.
The NSFG also documents large declines in formal instruction about birth control from 1995 to 2011-2013 falling from 87% to 60% of adolescent females and 81% to 55% of adolescent males.
Although formal instruction on birth control has significantly declined, 9 out of 10 adolescents report receiving formal instruction about STDs.
Click here for additional information about Sex Education in the United States.
Abortion Debate: Pro Choice or Pro Life?
YouTube Video: Moving Beyond Pro-Life vs. Pro-Choice Labels, You're "Not in Her Shoes" -- Planned Parenthood

The abortion debate is the ongoing controversy surrounding the moral and legal status of induced abortion. The sides involved in the debate are the self-described "pro-choice" movement (emphasizing the right of women to decide whether to terminate a pregnancy) and the self-described "pro-life" movement (emphasizing the right of the embryo or fetus to gestate to term and be born).
Both terms are considered loaded in mainstream media, where terms such as "abortion rights" or "anti-abortion" are generally preferred. Each movement has, with varying results, sought to influence public opinion and to attain legal support for its position, with small numbers of anti-abortion advocates sometimes using violence.
For many people, abortion is essentially a moral issue, concerning the commencement of human conception, the rights of the fetus, and a woman's rights over her own body. The debate has become a political and legal issue in some countries with anti-abortion campaigners seeking to enact, maintain and expand anti-abortion laws, while abortion rights campaigners seeking the repeal or easing of such laws while improving access to abortion.
Abortion laws vary considerably between jurisdictions, ranging from outright prohibition of the procedure to few limitations on it. Availability of safe abortion also varies across the world.
Click on any of the blue hyperlinks below for further amplification:
Both terms are considered loaded in mainstream media, where terms such as "abortion rights" or "anti-abortion" are generally preferred. Each movement has, with varying results, sought to influence public opinion and to attain legal support for its position, with small numbers of anti-abortion advocates sometimes using violence.
For many people, abortion is essentially a moral issue, concerning the commencement of human conception, the rights of the fetus, and a woman's rights over her own body. The debate has become a political and legal issue in some countries with anti-abortion campaigners seeking to enact, maintain and expand anti-abortion laws, while abortion rights campaigners seeking the repeal or easing of such laws while improving access to abortion.
Abortion laws vary considerably between jurisdictions, ranging from outright prohibition of the procedure to few limitations on it. Availability of safe abortion also varies across the world.
Click on any of the blue hyperlinks below for further amplification:
- Overview
- Terminology
- Political debate:
- Moral issues:
- Personhood
- Fetal pain
- Arguments for abortion rights which do not depend on fetal non-personhood
- Arguments against the right to abortion:
- Other factors:
- See also:
- Abortion law
- Bubble zone laws
- Conscience clause (medical)
- Embryonic stem cell research
- Equal Protection Clause
- Paper Abortion
- Feticide
- Late-term abortion
- Opposition to the legalization of abortion
- Reproductive rights
- Roe effect
- Roe v. Wade
- Societal attitudes towards abortion
- Support for the legalization of abortion
- Philosophical aspects of the abortion debate
- Beginning of human life
Human Reproduction including the Role of Estrogen and Testosterone
YouTube Video: The Human Reproduction | Educational Video for Kids
YouTube Video: FEMALE REPRODUCTIVE SYSTEM
YouTube Video: MALE REPRODUCTIVE SYSTEM
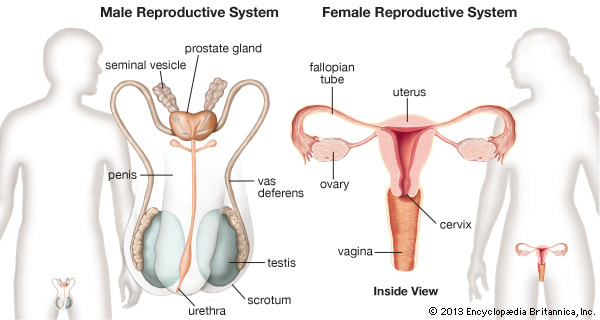
Preceding Human Reproduction, Estrogen is responsible for female reproductive development and regulation:
Estrogen is the primary female sex hormone as well as a medication. It is responsible for the development and regulation of the female reproductive system and secondary sex characteristics. Estrogen may also refer to any substance, natural or synthetic, that mimics the effects of the natural hormone. The estrane steroid estradiol is the most potent and prevalent endogenous estrogen, although several metabolites of estradiol also have estrogenic hormonal activity.
Estrogens are used as medications as part of some oral contraceptives, in hormone replacement therapy for postmenopausal, hypogonadal, and transgender women, and in the treatment of certain hormone-sensitive cancers like prostate cancer and breast cancer.
They are one of three types of sex hormones, the others being androgens/anabolic steroids like testosterone and progestogens like progesterone.
Estrogens are synthesized in all vertebrates as well as some insects. Their presence in both vertebrates and insects suggests that estrogenic sex hormones have an ancient evolutionary history.
The three major naturally occurring forms of estrogen in women are estrone (E1), estradiol (E2), and estriol (E3). Another type of estrogen called estetrol (E4) is produced only during pregnancy.
Quantitatively, estrogens circulate at lower levels than androgens in both men and women. While estrogen levels are significantly lower in males compared to females, estrogens nevertheless also have important physiological roles in males.
Like all steroid hormones, estrogens readily diffuse across the cell membrane. Once inside the cell, they bind to and activate estrogen receptors (ERs) which in turn modulate the expression of many genes. Additionally, estrogens bind to and activate rapid-signaling membrane estrogen receptors (mERs), such as GPER (GPR30).
Click here for more about the female hormone Estrogen.
___________________________________________________________________________
Testosterone is the primary male sex hormone and an anabolic steroid. In men, testosterone plays a key role in the development of male reproductive tissues such as the testis and prostate, as well as promoting secondary sexual characteristics such as increased muscle and bone mass, and the growth of body hair.
In addition, testosterone is involved in health and well-being, and the prevention of osteoporosis. Insufficient levels of testosterone in men may lead to abnormalities including frailty and bone loss.
Testosterone is also used as a medication to treat male hypogonadism and certain types of breast cancer. Since testosterone levels gradually decrease as men age, synthetic testosterone is sometimes prescribed to older men to counteract this deficiency.
Testosterone is a steroid from the androstane class containing a keto and hydroxyl groups at the three and seventeen positions respectively. It is biosynthesized in several steps from cholesterol and is converted in the liver to inactive metabolites. It exerts its action through binding to and activation of the androgen receptor.
In humans and most other vertebrates, testosterone is secreted primarily by the testicles of males and, to a lesser extent, the ovaries of females. Small amounts are also secreted by the adrenal glands. On average, in adult males, levels of testosterone are about 7–8 times as great as in adult females. As the metabolic consumption of testosterone in males is greater, the daily production is about 20 times greater in men. Females are also more sensitive to the hormone.
Click here for more about the male hormone, Testosterone.
___________________________________________________________________________
Human Reproduction:
Human reproduction is any form of sexual reproduction resulting in human fertilization, typically involving sexual intercourse between a man and a woman. During sexual intercourse, the interaction between the male and female reproductive systems results in fertilization of the woman's ovum by the man's sperm. These are specialized reproductive cells called gametes, created in a process called meiosis.
While normal cells contains 46 chromosomes, 23 pairs, gamete cells only contain 23 chromosomes, and it is when these two cells merge into one zygote cell that genetic recombination occurs and the new zygote contains 23 chromosomes from each parent, giving them 23 pairs. After a gestation period, typically for nine months, is followed by childbirth. The fertilization of the ovum may be achieved by artificial insemination methods, which do not involve sexual intercourse.
Anatomy
Human Male:
For more details on this topic, see Human male reproductive system.
The male reproductive system contains two main divisions: the testes where sperm are produced, and the penis. In humans, both of these organs are outside the abdominal cavity.
Having the testes outside the abdomen facilitates temperature regulation of the sperm, which require specific temperatures to survive about 2-3 °C less than the normal body temperature i.e. 37 °C.
In particular, the extraperitoneal location of the testes may result in a 2-fold reduction in the heat-induced contribution to the spontaneous mutation rate in male germinal tissues compared to tissues at 37 °C. If the testicles remain too close to the body, it is likely that the increase in temperature will harm the spermatozoa formation, making conception more difficult. This is why the testes are carried in an external pouch viz. scrotum rather than within the abdomen; they normally remain slightly cooler than body temperature, facilitating sperm production.
Human female:
For more details on this topic, see Female reproductive system.
The female reproductive system likewise contains two main divisions: the vagina and the Ovum which is the equivalent to the males testes.
The fertilization of the ovum with the sperm occurs at the ampullary-isthimic junction only. That is why not all intercourse results in pregnancy. The ovum meets with Spermatozoon, a sperm may penetrate and merge with the egg, fertilizing it with the help of certain hydrolytic enzymes present in the acrosome.
The fertilization usually occurs in the oviducts, but can happen in the uterus itself. The zygote then becomes implanted in the lining of the uterus, where it begins the processes of embryogenesis and morphogenesis. When the fetus is developed enough to survive outside of the uterus, the cervix dilates and contractions of the uterus propel it through the birth canal, which is the vagina.
The ova, which are the female sex cells, are much larger than the spermatozoon and are normally formed within the ovaries of the female fetus before its birth. They are mostly fixed in location within the ovary until their transit to the uterus, and contain nutrients for the later zygote and embryo. Over a regular interval, in response to hormonal signals, a process of oogenesis matures one ovum which is released and sent down the Fallopian tube. If not fertilized, this egg is flushed out of the system through menstruation.
Process:
Human reproduction normally begins with copulation, followed by nine months of pregnancy before childbirth, though it may be achieved through artificial insemination. Many years of parental care are required before a human child becomes independent, typically between twelve and eighteen or more. Pregnancy can be avoided with the use of contraceptives such as condoms and Intrauterine devices.
Copulation:
Main article: Sexual intercourse
Human reproduction takes place as internal fertilization by sexual intercourse. During this process, the male inserts his penis, which needs to be erect, into the female's vagina, and then either partner initiates rhythmic pelvic thrusts until the male ejaculates semen, which contains sperm, into the vaginal canal. This process is also known as "coitus", "mating", "having sex", or, euphemistically, "making love".
The sperm and the ovum are known as gametes (each containing half the genetic information of the parent, created through meiosis). The sperm (being one of approximately 250 million sperm in a typical male ejaculation) travels through the vagina and cervix into the uterus or Fallopian tubes.
Only 1 in 14 million of the ejaculated sperm will reach the Fallopian tube. The egg simultaneously moves through the Fallopian tube away from the ovary. One of the sperm encounters, penetrates and fertilizes the ovum, creating a zygote.
Upon fertilization and implantation, gestation of the fetus then occurs within the female's uterus.
Pregnancy:
Main article: Pregnancy
Pregnancy is the period of time during which the fetus develops, dividing via mitosis inside the female.
During this time, the fetus receives all of its nutrition and oxygenated blood from the female, filtered through the placenta, which is attached to the fetus' abdomen via an umbilical cord.
This drain of nutrients can be quite taxing on the female, who is required to ingest slightly higher levels of calories. In addition, certain vitamins and other nutrients are required in greater quantities than normal, often creating abnormal eating habits. Gestation period is about 266 days in humans.
While in the uterus, the baby first endures a very brief zygote stage, then the embryonic stage, which is marked by the development of major organs and lasts for approximately eight weeks, then the fetal stage, which revolves around the development of bone cells while the fetus continues to grow in size.
Birth:
Main article: Childbirth
Once the fetus is sufficiently developed, chemical signals begin the process of birth, which begins with the fetus being pushed out of the birthing canal. The newborn, which is called an infant in humans, should typically begin respiration on its own shortly after birth. Not long after, the placenta eventually falls off on its own. The person assisting the birth may also sever the umbilical cord.
Parental Care:
Main article: Parenting
A human baby is nearly helpless and the growing child requires high levels of parental care for many years. One important type of early parental care is lactation, feeding the baby milk from the mother's mammary glands in her breasts.
See Also:
Estrogen is the primary female sex hormone as well as a medication. It is responsible for the development and regulation of the female reproductive system and secondary sex characteristics. Estrogen may also refer to any substance, natural or synthetic, that mimics the effects of the natural hormone. The estrane steroid estradiol is the most potent and prevalent endogenous estrogen, although several metabolites of estradiol also have estrogenic hormonal activity.
Estrogens are used as medications as part of some oral contraceptives, in hormone replacement therapy for postmenopausal, hypogonadal, and transgender women, and in the treatment of certain hormone-sensitive cancers like prostate cancer and breast cancer.
They are one of three types of sex hormones, the others being androgens/anabolic steroids like testosterone and progestogens like progesterone.
Estrogens are synthesized in all vertebrates as well as some insects. Their presence in both vertebrates and insects suggests that estrogenic sex hormones have an ancient evolutionary history.
The three major naturally occurring forms of estrogen in women are estrone (E1), estradiol (E2), and estriol (E3). Another type of estrogen called estetrol (E4) is produced only during pregnancy.
Quantitatively, estrogens circulate at lower levels than androgens in both men and women. While estrogen levels are significantly lower in males compared to females, estrogens nevertheless also have important physiological roles in males.
Like all steroid hormones, estrogens readily diffuse across the cell membrane. Once inside the cell, they bind to and activate estrogen receptors (ERs) which in turn modulate the expression of many genes. Additionally, estrogens bind to and activate rapid-signaling membrane estrogen receptors (mERs), such as GPER (GPR30).
Click here for more about the female hormone Estrogen.
___________________________________________________________________________
Testosterone is the primary male sex hormone and an anabolic steroid. In men, testosterone plays a key role in the development of male reproductive tissues such as the testis and prostate, as well as promoting secondary sexual characteristics such as increased muscle and bone mass, and the growth of body hair.
In addition, testosterone is involved in health and well-being, and the prevention of osteoporosis. Insufficient levels of testosterone in men may lead to abnormalities including frailty and bone loss.
Testosterone is also used as a medication to treat male hypogonadism and certain types of breast cancer. Since testosterone levels gradually decrease as men age, synthetic testosterone is sometimes prescribed to older men to counteract this deficiency.
Testosterone is a steroid from the androstane class containing a keto and hydroxyl groups at the three and seventeen positions respectively. It is biosynthesized in several steps from cholesterol and is converted in the liver to inactive metabolites. It exerts its action through binding to and activation of the androgen receptor.
In humans and most other vertebrates, testosterone is secreted primarily by the testicles of males and, to a lesser extent, the ovaries of females. Small amounts are also secreted by the adrenal glands. On average, in adult males, levels of testosterone are about 7–8 times as great as in adult females. As the metabolic consumption of testosterone in males is greater, the daily production is about 20 times greater in men. Females are also more sensitive to the hormone.
Click here for more about the male hormone, Testosterone.
___________________________________________________________________________
Human Reproduction:
Human reproduction is any form of sexual reproduction resulting in human fertilization, typically involving sexual intercourse between a man and a woman. During sexual intercourse, the interaction between the male and female reproductive systems results in fertilization of the woman's ovum by the man's sperm. These are specialized reproductive cells called gametes, created in a process called meiosis.
While normal cells contains 46 chromosomes, 23 pairs, gamete cells only contain 23 chromosomes, and it is when these two cells merge into one zygote cell that genetic recombination occurs and the new zygote contains 23 chromosomes from each parent, giving them 23 pairs. After a gestation period, typically for nine months, is followed by childbirth. The fertilization of the ovum may be achieved by artificial insemination methods, which do not involve sexual intercourse.
Anatomy
Human Male:
For more details on this topic, see Human male reproductive system.
The male reproductive system contains two main divisions: the testes where sperm are produced, and the penis. In humans, both of these organs are outside the abdominal cavity.
Having the testes outside the abdomen facilitates temperature regulation of the sperm, which require specific temperatures to survive about 2-3 °C less than the normal body temperature i.e. 37 °C.
In particular, the extraperitoneal location of the testes may result in a 2-fold reduction in the heat-induced contribution to the spontaneous mutation rate in male germinal tissues compared to tissues at 37 °C. If the testicles remain too close to the body, it is likely that the increase in temperature will harm the spermatozoa formation, making conception more difficult. This is why the testes are carried in an external pouch viz. scrotum rather than within the abdomen; they normally remain slightly cooler than body temperature, facilitating sperm production.
Human female:
For more details on this topic, see Female reproductive system.
The female reproductive system likewise contains two main divisions: the vagina and the Ovum which is the equivalent to the males testes.
The fertilization of the ovum with the sperm occurs at the ampullary-isthimic junction only. That is why not all intercourse results in pregnancy. The ovum meets with Spermatozoon, a sperm may penetrate and merge with the egg, fertilizing it with the help of certain hydrolytic enzymes present in the acrosome.
The fertilization usually occurs in the oviducts, but can happen in the uterus itself. The zygote then becomes implanted in the lining of the uterus, where it begins the processes of embryogenesis and morphogenesis. When the fetus is developed enough to survive outside of the uterus, the cervix dilates and contractions of the uterus propel it through the birth canal, which is the vagina.
The ova, which are the female sex cells, are much larger than the spermatozoon and are normally formed within the ovaries of the female fetus before its birth. They are mostly fixed in location within the ovary until their transit to the uterus, and contain nutrients for the later zygote and embryo. Over a regular interval, in response to hormonal signals, a process of oogenesis matures one ovum which is released and sent down the Fallopian tube. If not fertilized, this egg is flushed out of the system through menstruation.
Process:
Human reproduction normally begins with copulation, followed by nine months of pregnancy before childbirth, though it may be achieved through artificial insemination. Many years of parental care are required before a human child becomes independent, typically between twelve and eighteen or more. Pregnancy can be avoided with the use of contraceptives such as condoms and Intrauterine devices.
Copulation:
Main article: Sexual intercourse
Human reproduction takes place as internal fertilization by sexual intercourse. During this process, the male inserts his penis, which needs to be erect, into the female's vagina, and then either partner initiates rhythmic pelvic thrusts until the male ejaculates semen, which contains sperm, into the vaginal canal. This process is also known as "coitus", "mating", "having sex", or, euphemistically, "making love".
The sperm and the ovum are known as gametes (each containing half the genetic information of the parent, created through meiosis). The sperm (being one of approximately 250 million sperm in a typical male ejaculation) travels through the vagina and cervix into the uterus or Fallopian tubes.
Only 1 in 14 million of the ejaculated sperm will reach the Fallopian tube. The egg simultaneously moves through the Fallopian tube away from the ovary. One of the sperm encounters, penetrates and fertilizes the ovum, creating a zygote.
Upon fertilization and implantation, gestation of the fetus then occurs within the female's uterus.
Pregnancy:
Main article: Pregnancy
Pregnancy is the period of time during which the fetus develops, dividing via mitosis inside the female.
During this time, the fetus receives all of its nutrition and oxygenated blood from the female, filtered through the placenta, which is attached to the fetus' abdomen via an umbilical cord.
This drain of nutrients can be quite taxing on the female, who is required to ingest slightly higher levels of calories. In addition, certain vitamins and other nutrients are required in greater quantities than normal, often creating abnormal eating habits. Gestation period is about 266 days in humans.
While in the uterus, the baby first endures a very brief zygote stage, then the embryonic stage, which is marked by the development of major organs and lasts for approximately eight weeks, then the fetal stage, which revolves around the development of bone cells while the fetus continues to grow in size.
Birth:
Main article: Childbirth
Once the fetus is sufficiently developed, chemical signals begin the process of birth, which begins with the fetus being pushed out of the birthing canal. The newborn, which is called an infant in humans, should typically begin respiration on its own shortly after birth. Not long after, the placenta eventually falls off on its own. The person assisting the birth may also sever the umbilical cord.
Parental Care:
Main article: Parenting
A human baby is nearly helpless and the growing child requires high levels of parental care for many years. One important type of early parental care is lactation, feeding the baby milk from the mother's mammary glands in her breasts.
See Also:
- Antinatalism
- Evolution of sexual reproduction
- Female infertility
- Human Reproduction (journal)
- Journal of Human Reproductive Sciences
- Male infertility
- Natalism
- Reproduction
- Reproductive system
Human Sex Pheromones
YouTube Video: Do Athena Pheromones work? -ABC 20/20 Twins Experiment
Pictured Below: Do Pheromone Sprays Really Work To Attract Women?
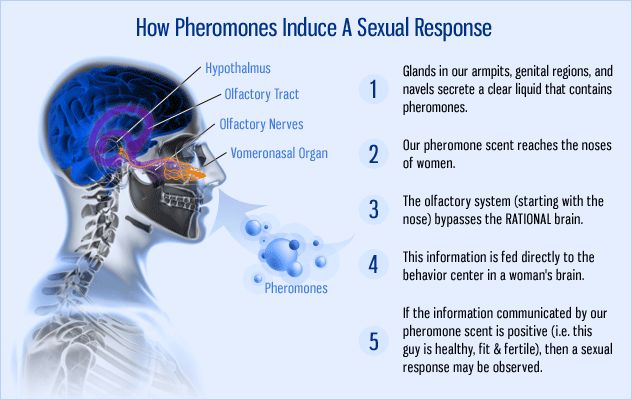
No study has led to the isolation of true human sex pheromones, though various researchers have investigated the possibility of their existence.
Sex pheromones are chemical (olfactory) signals, pheromones, released by an organism to attract an individual of the opposite sex, encourage them to mate with them, or perform some other function closely related with sexual reproduction. While humans are highly dependent upon visual cues, when in close proximity, smells also play a role in socio-sexual behaviors.
An inherent difficulty in studying human pheromones is the need for cleanliness and odorlessness in human participants. Experiments have focused on three classes of putative human pheromones: axillary steroids, vaginal aliphatic acids, and stimulators of the vomeronasal organ.
Axillary steroids are produced by the testes, ovaries, apocrine glands and adrenal glands. These chemicals are not biologically active until puberty when sex steroids influence their activity.
The activity change during puberty suggest that humans communicate through odors.Several axillary steroids have been described as possible human pheromones:
Androstenol is the putative female pheromone. In a 1978 study by Kirk-Smith, people wearing surgical masks treated with androstenol or untreated were shown pictures of people, animals and buildings and asked to rate the pictures on attractiveness.
Individuals with their masks treated with androstenol rated their photographs as being "warmer" and "more friendly". The best-known case study involves the synchronization of menstrual cycles among women based on unconscious odor cues, the McClintock effect, named after the primary investigator, Martha McClintock, of the University of Chicago.
A group of women were exposed to a whiff of perspiration from other women. Depending on the time in the month the sweat was collected (before, during, or after ovulation), there was an association with the recipient woman's menstrual cycle to speed up or slow down. The 1971 study proposed two types of pheromone involved: "One, produced prior to ovulation, shortens the ovarian cycle; and the second, produced just at ovulation, lengthens the cycle".
However, recent studies and reviews of the methodology have called the validity of her results into question.
Androstenone is postulated to be secreted only by men as an attractant for women and is also thought to affect their mood positively. It seems to have different effects on women, depending on where a female is in her menstrual cycle, with the highest sensitivity to it during ovulation.
In 1983, study participants exposed to androstenone were shown to undergo changes in skin conductance. Androstenone has been found to be perceived as more pleasant to women at a woman’s time of ovulation. It is hypothesized that this may be a way for a male to detect an ovulating female who would be more willing to be involved in sexual interaction.
See also:
Sex pheromones are chemical (olfactory) signals, pheromones, released by an organism to attract an individual of the opposite sex, encourage them to mate with them, or perform some other function closely related with sexual reproduction. While humans are highly dependent upon visual cues, when in close proximity, smells also play a role in socio-sexual behaviors.
An inherent difficulty in studying human pheromones is the need for cleanliness and odorlessness in human participants. Experiments have focused on three classes of putative human pheromones: axillary steroids, vaginal aliphatic acids, and stimulators of the vomeronasal organ.
Axillary steroids are produced by the testes, ovaries, apocrine glands and adrenal glands. These chemicals are not biologically active until puberty when sex steroids influence their activity.
The activity change during puberty suggest that humans communicate through odors.Several axillary steroids have been described as possible human pheromones:
Androstenol is the putative female pheromone. In a 1978 study by Kirk-Smith, people wearing surgical masks treated with androstenol or untreated were shown pictures of people, animals and buildings and asked to rate the pictures on attractiveness.
Individuals with their masks treated with androstenol rated their photographs as being "warmer" and "more friendly". The best-known case study involves the synchronization of menstrual cycles among women based on unconscious odor cues, the McClintock effect, named after the primary investigator, Martha McClintock, of the University of Chicago.
A group of women were exposed to a whiff of perspiration from other women. Depending on the time in the month the sweat was collected (before, during, or after ovulation), there was an association with the recipient woman's menstrual cycle to speed up or slow down. The 1971 study proposed two types of pheromone involved: "One, produced prior to ovulation, shortens the ovarian cycle; and the second, produced just at ovulation, lengthens the cycle".
However, recent studies and reviews of the methodology have called the validity of her results into question.
Androstenone is postulated to be secreted only by men as an attractant for women and is also thought to affect their mood positively. It seems to have different effects on women, depending on where a female is in her menstrual cycle, with the highest sensitivity to it during ovulation.
In 1983, study participants exposed to androstenone were shown to undergo changes in skin conductance. Androstenone has been found to be perceived as more pleasant to women at a woman’s time of ovulation. It is hypothesized that this may be a way for a male to detect an ovulating female who would be more willing to be involved in sexual interaction.
See also:
Sexually Transmitted Diseases (STD)
YouTube Video: Let's Talk about Sexual Health (by the CDC)
Pictured below: The most commonly sexually transmitted diseases
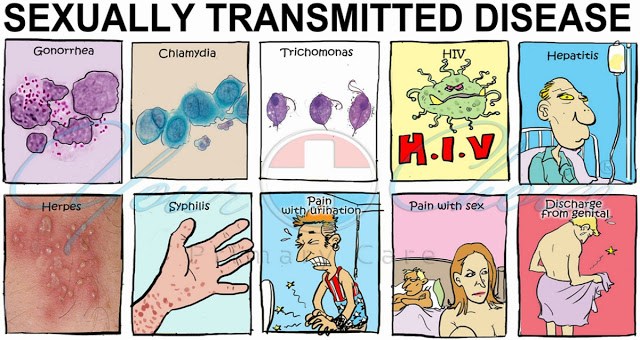
Sexually transmitted infections (STI), also referred to as sexually transmitted diseases (STD) and venereal diseases (VD), are infections that are commonly spread by sexual activity, especially vaginal intercourse, anal sex and oral sex.
Many times STIs initially do not cause symptoms. This results in a greater risk of passing the disease on to others. Symptoms and signs of disease may include:
STIs can be transmitted to an infant before or during childbirth and may result in poor outcomes for the baby. Some STIs may cause problems with the ability to get pregnant.
More than 30 different bacteria, viruses, and parasites can be transmitted through sexual activity. Bacterial STIs include chlamydia, gonorrhea, and syphilis.
Viral STIs include genital herpes, HIV/AIDS, and genital warts.
Parasitic STIs include trichomoniasis.
While usually spread by sex, some STIs can be spread by non-sexual contact with donor tissue, blood, breastfeeding, or during childbirth. STI diagnostic tests are usually easily available in the developed world, but this is often not the case in the developing world.
The most effective way of preventing STIs is by not having sex. Some vaccinations may also decrease the risk of certain infections including hepatitis B and some types of HPV.
Safer sex practices such as use of condoms, having a smaller number of sexual partners, and being in a relationship where each person only has sex with the other also decreases the risk. Circumcision in males may be effective to prevent some infections.
Most STIs are treatable or curable. During school, comprehensive sex education may also be useful. Of the most common infections, syphilis, gonorrhea, chlamydia, trichomoniasis are curable, while herpes, hepatitis B, HIV/AIDS, and HPV are treatable but not curable.
Resistance to certain antibiotics is developing among some organisms such as gonorrhea.
In 2015, about 1.1 billion people had STIs other than HIV/AIDS:
STIs other than HIV resulted in 108,000 deaths in 2015. In the United States there were 19 million new cases of sexually transmitted infections in 2010.
Historical documentation of STIs date back to at least the Ebers papyrus around 1550 BC and the Old Testament. There is often shame and stigma associated with these infections. The term sexually transmitted infection is generally preferred over sexually transmitted disease or venereal disease, as it includes those who do not have symptomatic disease
Classification:
Until the 1990s, STIs were commonly known as venereal diseases, the word venereal being derived from the Latin word venereus, and meaning relating to sexual intercourse or desire, ultimately derived from Venus, the Roman goddess of love. STIs have been euphemistically referred to as "blood diseases" and "social diseases" in the past.
The World Health Organization (WHO) has recommended the more inclusive term sexually transmitted infection since 1999. Public health officials originally introduced the term sexually transmitted infection, which clinicians are increasingly using alongside the term sexually transmitted disease in order to distinguish it from the former
Signs and Symptoms:
Not all STIs are symptomatic, and symptoms may not appear immediately after infection. In some instances a disease can be carried with no symptoms, which leaves a greater risk of passing the disease on to others. Depending on the disease, some untreated STIs can lead to infertility, chronic pain or even death.
The presence of an STI in prepubescent children may indicate sexual abuse.
Click on any of the following blue hyperlinks for more about Sexually Transmitted Diseases:
Many times STIs initially do not cause symptoms. This results in a greater risk of passing the disease on to others. Symptoms and signs of disease may include:
STIs can be transmitted to an infant before or during childbirth and may result in poor outcomes for the baby. Some STIs may cause problems with the ability to get pregnant.
More than 30 different bacteria, viruses, and parasites can be transmitted through sexual activity. Bacterial STIs include chlamydia, gonorrhea, and syphilis.
Viral STIs include genital herpes, HIV/AIDS, and genital warts.
Parasitic STIs include trichomoniasis.
While usually spread by sex, some STIs can be spread by non-sexual contact with donor tissue, blood, breastfeeding, or during childbirth. STI diagnostic tests are usually easily available in the developed world, but this is often not the case in the developing world.
The most effective way of preventing STIs is by not having sex. Some vaccinations may also decrease the risk of certain infections including hepatitis B and some types of HPV.
Safer sex practices such as use of condoms, having a smaller number of sexual partners, and being in a relationship where each person only has sex with the other also decreases the risk. Circumcision in males may be effective to prevent some infections.
Most STIs are treatable or curable. During school, comprehensive sex education may also be useful. Of the most common infections, syphilis, gonorrhea, chlamydia, trichomoniasis are curable, while herpes, hepatitis B, HIV/AIDS, and HPV are treatable but not curable.
Resistance to certain antibiotics is developing among some organisms such as gonorrhea.
In 2015, about 1.1 billion people had STIs other than HIV/AIDS:
- About 500 million were infected with either syphilis, gonorrhea, chlamydia or trichomoniasis.
- At least an additional 530 million people have genital herpes
- and 290 million women have human papillomavirus.
STIs other than HIV resulted in 108,000 deaths in 2015. In the United States there were 19 million new cases of sexually transmitted infections in 2010.
Historical documentation of STIs date back to at least the Ebers papyrus around 1550 BC and the Old Testament. There is often shame and stigma associated with these infections. The term sexually transmitted infection is generally preferred over sexually transmitted disease or venereal disease, as it includes those who do not have symptomatic disease
Classification:
Until the 1990s, STIs were commonly known as venereal diseases, the word venereal being derived from the Latin word venereus, and meaning relating to sexual intercourse or desire, ultimately derived from Venus, the Roman goddess of love. STIs have been euphemistically referred to as "blood diseases" and "social diseases" in the past.
The World Health Organization (WHO) has recommended the more inclusive term sexually transmitted infection since 1999. Public health officials originally introduced the term sexually transmitted infection, which clinicians are increasingly using alongside the term sexually transmitted disease in order to distinguish it from the former
Signs and Symptoms:
Not all STIs are symptomatic, and symptoms may not appear immediately after infection. In some instances a disease can be carried with no symptoms, which leaves a greater risk of passing the disease on to others. Depending on the disease, some untreated STIs can lead to infertility, chronic pain or even death.
The presence of an STI in prepubescent children may indicate sexual abuse.
Click on any of the following blue hyperlinks for more about Sexually Transmitted Diseases:
- Cause
- Pathophysiology
- Prevention
- Screening
- Diagnosis
- Management
- Epidemiology
- History
- Other names or slang terms
- Plants
- See also:
Sexual Orientation Including a List of Well-known Gay, Lesbian or Bisexual People
YouTube Video by Ellen Celebrating the 20th Anniversary of Her 'Coming Out' Episode
Pictured: (L) Former Congressman Barney Frank (R) MSNBC Host Rachel Maddow
Click here for a List of Well-known Gay, Lesbian or Bisexual People.
Sexual orientation is an enduring pattern of romantic or sexual attraction (or a combination of these) to persons of the opposite sex or gender, the same sex or gender, or to both sexes or more than one gender.
These attractions are generally subsumed under heterosexuality, homosexuality, and bisexuality, while asexuality (the lack of sexual attraction to others) is sometimes identified as the fourth category.
These categories are aspects of the more nuanced nature of sexual identity and terminology.
For example, people may use other labels, such as pansexual or polysexual, or none at all.
According to the American Psychological Association, sexual orientation "also refers to a person's sense of identity based on those attractions, related behaviors, and membership in a community of others who share those attractions". Androphilia and gynephilia are terms used in behavioral science to describe sexual orientation as an alternative to a gender binary conceptualization. Androphilia describes sexual attraction to masculinity; gynephilia describes the sexual attraction to femininity.
The term sexual preference largely overlaps with sexual orientation, but is generally distinguished in psychological research. A person who identifies as bisexual, for example, may sexually prefer one sex over the other. Sexual preference may also suggest a degree of voluntary choice, whereas the scientific consensus is that sexual orientation is not a choice.
Scientists do not know the exact causes of sexual orientation, but they believe that it is caused by a complex interplay of genetic, hormonal, and environmental influences.
They favor biologically-based theories,which point to genetic factors, the early uterine environment, both, or the inclusion of genetic and social factors. There is no substantive evidence which suggests parenting or early childhood experiences play a role when it comes to sexual orientation. Research over several decades has demonstrated that sexual orientation ranges along a continuum, from exclusive attraction to the opposite sex to exclusive attraction to the same sex.
Sexual orientation is reported primarily within biology and psychology (including sexology), but it is also a subject area in anthropology, history (including social constructionism), and law, and there are other explanations that relate to sexual orientation and culture.
Click on any of the following blue hyperlinks for more about Sexual Orientation:
Sexual orientation is an enduring pattern of romantic or sexual attraction (or a combination of these) to persons of the opposite sex or gender, the same sex or gender, or to both sexes or more than one gender.
These attractions are generally subsumed under heterosexuality, homosexuality, and bisexuality, while asexuality (the lack of sexual attraction to others) is sometimes identified as the fourth category.
These categories are aspects of the more nuanced nature of sexual identity and terminology.
For example, people may use other labels, such as pansexual or polysexual, or none at all.
According to the American Psychological Association, sexual orientation "also refers to a person's sense of identity based on those attractions, related behaviors, and membership in a community of others who share those attractions". Androphilia and gynephilia are terms used in behavioral science to describe sexual orientation as an alternative to a gender binary conceptualization. Androphilia describes sexual attraction to masculinity; gynephilia describes the sexual attraction to femininity.
The term sexual preference largely overlaps with sexual orientation, but is generally distinguished in psychological research. A person who identifies as bisexual, for example, may sexually prefer one sex over the other. Sexual preference may also suggest a degree of voluntary choice, whereas the scientific consensus is that sexual orientation is not a choice.
Scientists do not know the exact causes of sexual orientation, but they believe that it is caused by a complex interplay of genetic, hormonal, and environmental influences.
They favor biologically-based theories,which point to genetic factors, the early uterine environment, both, or the inclusion of genetic and social factors. There is no substantive evidence which suggests parenting or early childhood experiences play a role when it comes to sexual orientation. Research over several decades has demonstrated that sexual orientation ranges along a continuum, from exclusive attraction to the opposite sex to exclusive attraction to the same sex.
Sexual orientation is reported primarily within biology and psychology (including sexology), but it is also a subject area in anthropology, history (including social constructionism), and law, and there are other explanations that relate to sexual orientation and culture.
Click on any of the following blue hyperlinks for more about Sexual Orientation:
- Definitions and distinguishing from sexual identity and behavior
- Causes
- Biology
- Genetic factors
Hormones
Birth order
- Genetic factors
- Environmental factors
- Influences: professional organizations' statements
- Biology
- Efforts to change sexual orientation
- Assessment and measurement
- Culture
- Demographics
- Social constructionism and Western societies
- Law, politics and theology
- See also:
- Romantic orientation
- Ascribed characteristics
- Bisexuality in the United States
- Genetic diagnosis of intersex
- Hate crime and Homophobia
- History of gay men in the United States
- History of lesbianism in the United States
- LGBT (Lesbian, Gay, Bisexual, and Transgender)
- List of anti-discrimination acts
- LGBT rights by country or territory
- Fundamental Rights Agency
- Human male sexuality, including non-western perspectives on sexual orientation
- Marriage and Same-sex marriage
- Sexual orientation and military service
- Sexual orientation hypothesis
- Terminology of homosexuality
- Sociosexual orientation
- Sexual orientation and gender identity at the United Nations
- Sexual Orientation FAQ
- American Psychological Association: Answers to Your Questions About Sexual Orientation and Homosexuality
- Brain gender: prostaglandins have their say
- Etiology on glbtq.com
- Magnus Hirschfeld Archive of Sexology at the Humboldt University in Berlin
- Survivor bashing – bias motivated hate crimes
- The Science Of Sexual Orientation
- The SexEdLibrary
- BORN FREE AND EQUAL - Sexual orientation and gender identity in international human rights law
- Policies: Australia
- United States
- American Medical Association
- American Medical Student Association
- American Psychological Association: for public or educators
- Catholic Medical Association
Gender Equality
YouTube Video: Women's March 2018 Best Moments: Thousands Of Women March Around The World | TIME
Pictured below: Gender Equality Index

[Your Website Host: the subject of feminism is comprehensively covered under the separate web page "Ladies First".]
Gender equality, also known as sexual equality, is the state of equal ease of access to resources and opportunities regardless of gender, including economic participation and decision-making; and the state of valuing different behaviors, aspirations and needs equally, regardless of gender.
"Gender equality, equality between men and women, entails the concept that all human beings, both men and women, are free to develop their personal abilities and make choices without the limitations set by stereotypes, rigid gender roles and prejudices.
Gender equality means that the different behavior, aspirations and needs of women and men are considered, valued and favored equally. It does not mean that women and men have to become the same, but that their rights, responsibilities and opportunities will not depend on whether they are born male or female.
Gender equity means fairness of treatment for women and men, according to their respective needs. This may include equal treatment or treatment that is different but which is considered equivalent in terms of rights, benefits, obligations and opportunities."
— ABC Of Women Worker's Rights And Gender Equality, ILO, 2000. p. 48.
Gender equality is the goal, while gender neutrality and gender equity are practices and ways of thinking that help in achieving the goal. Gender parity, which is used to measure gender balance in a given situation, can aid in achieving gender equality but is not the goal in and of itself. Gender equality is more than equal representation, it is strongly tied to women's rights, and often requires policy changes.
As of 2017, the global movement for gender equality has not incorporated the proposition of genders besides women and men, or gender identities outside of the gender binary.
UNICEF says gender equality "means that women and men, and girls and boys, enjoy the same rights, resources, opportunities and protections. It does not require that girls and boys, or women and men, be the same, or that they be treated exactly alike."
On a global scale, achieving gender equality also requires eliminating harmful practices against women and girls, including:
UNFPA stated that, "despite many international agreements affirming their human rights, women are still much more likely than men to be poor and illiterate. They have less access to property ownership, credit, training and employment. They are far less likely than men to be politically active and far more likely to be victims of domestic violence."
As of 2017, gender equality is the fifth of seventeen sustainable development goals of the United Nations. Gender inequality is measured annually by the United Nations Development Programme's Human Development Reports.
Click on any of the following blue hyperlinks for more about Gender Equality:
Gender equality, also known as sexual equality, is the state of equal ease of access to resources and opportunities regardless of gender, including economic participation and decision-making; and the state of valuing different behaviors, aspirations and needs equally, regardless of gender.
"Gender equality, equality between men and women, entails the concept that all human beings, both men and women, are free to develop their personal abilities and make choices without the limitations set by stereotypes, rigid gender roles and prejudices.
Gender equality means that the different behavior, aspirations and needs of women and men are considered, valued and favored equally. It does not mean that women and men have to become the same, but that their rights, responsibilities and opportunities will not depend on whether they are born male or female.
Gender equity means fairness of treatment for women and men, according to their respective needs. This may include equal treatment or treatment that is different but which is considered equivalent in terms of rights, benefits, obligations and opportunities."
— ABC Of Women Worker's Rights And Gender Equality, ILO, 2000. p. 48.
Gender equality is the goal, while gender neutrality and gender equity are practices and ways of thinking that help in achieving the goal. Gender parity, which is used to measure gender balance in a given situation, can aid in achieving gender equality but is not the goal in and of itself. Gender equality is more than equal representation, it is strongly tied to women's rights, and often requires policy changes.
As of 2017, the global movement for gender equality has not incorporated the proposition of genders besides women and men, or gender identities outside of the gender binary.
UNICEF says gender equality "means that women and men, and girls and boys, enjoy the same rights, resources, opportunities and protections. It does not require that girls and boys, or women and men, be the same, or that they be treated exactly alike."
On a global scale, achieving gender equality also requires eliminating harmful practices against women and girls, including:
- sex trafficking,
- femicide,
- wartime sexual violence,
- and other oppression tactics.
UNFPA stated that, "despite many international agreements affirming their human rights, women are still much more likely than men to be poor and illiterate. They have less access to property ownership, credit, training and employment. They are far less likely than men to be politically active and far more likely to be victims of domestic violence."
As of 2017, gender equality is the fifth of seventeen sustainable development goals of the United Nations. Gender inequality is measured annually by the United Nations Development Programme's Human Development Reports.
Click on any of the following blue hyperlinks for more about Gender Equality:
- History
- Gender biases
- Efforts to fight inequality
- See also
- General issues
- Specific issues
- Laws
- Organizations and ministries
- Historical anecdotal reports
- Women and Gender Equality, the United Nations Internet Gateway on Gender Equality and Empowerment of Women.
- Gender Equality, an overview of the United Nations Development Program's work on Gender Equality.
- Gender issue -Significance in Watershed Management Programmes, Watershedpedia.
- GENDERNET International forum of gender experts working in support of Gender equality. Development Co-operation Directorate of the Organisation for Economic Co-operation and Development (OECD).
- OECD's Gender Initiative, an overview page which also links to wikiGENDER, the Gender equality project of the OECD Development Centre.
- The Local A news collection about Gender equality in Sweden.
- Egalitarian Jewish Services A Discussion Paper.
Menopause
- YouTube Video: What is perimenopause, and at what age does a woman experience it?
- YouTube Video about Menopause: Symptoms and Tips
- YouTube Video: Menopause is Misunderstood | Shirley Weir | TEDxGastownWomen
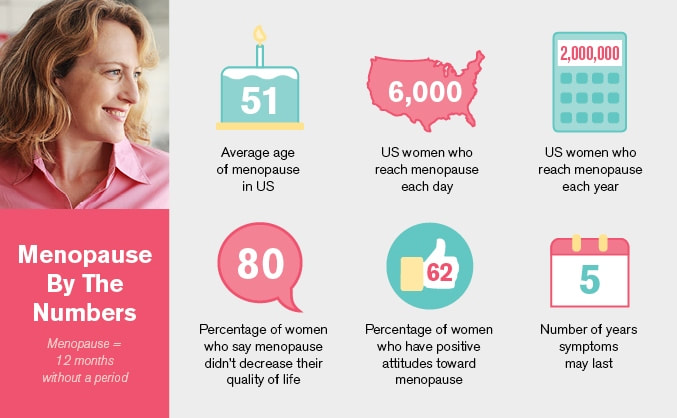
Menopause, also known as the climacteric, is the time in most women's lives when menstrual periods stop permanently, and they are no longer able to bear children. Menopause typically occurs between 49 and 52 years of age.
Medical professionals often define menopause as having occurred when a woman has not had any vaginal bleeding for a year. It may also be defined by a decrease in hormone production by the ovaries.
In those who have had surgery to remove their uterus but still have ovaries, menopause may be considered to have occurred at the time of the surgery or when their hormone levels fell.
Following the removal of the uterus, symptoms typically occur earlier, at an average of 45 years of age.
In the years before menopause, a woman's periods typically become irregular, which means that periods may be longer or shorter in duration or be lighter or heavier in the amount of flow. During this time, women often experience hot flashes; these typically last from 30 seconds to ten minutes and may be associated with shivering, sweating, and reddening of the skin.
Hot flashes often stop occurring after a year or two. Other symptoms may include vaginal dryness, trouble sleeping, and mood changes. The severity of symptoms varies between women. While menopause is often thought to be linked to an increase in heart disease, this primarily occurs due to increasing age and does not have a direct relationship with menopause.
In some women, problems that were present like endometriosis or painful periods will improve after menopause.
Menopause is usually a natural change. It can occur earlier in those who smoke tobacco. Other causes include surgery that removes both ovaries or some types of chemotherapy.
At the physiological level, menopause happens because of a decrease in the ovaries' production of the hormones estrogen and progesterone.
While typically not needed, a diagnosis of menopause can be confirmed by measuring hormone levels in the blood or urine. Menopause is the opposite of menarche, the time when a girl's periods start.
Specific treatment is not usually needed. Some symptoms, however, may be improved with treatment. With respect to hot flashes, avoiding smoking, caffeine, and alcohol is often recommended. Sleeping in a cool room and using a fan may help. The following medications may help:
Exercise may help with sleeping problems.
While MHT was once routinely prescribed, it is now only recommended in those with significant symptoms, as there are concerns about side effects. High-quality evidence for the effectiveness of alternative medicine has not been found. There is tentative evidence for phytoestrogens.
Signs and symptoms:
During early menopause transition, the menstrual cycles remain regular but the interval between cycles begins to lengthen. Hormone levels begin to fluctuate. Ovulation may not occur with each cycle.
The date of the final menstrual period is usually taken as the point when menopause has occurred. During the menopausal transition and after menopause, women can experience a wide range of symptoms.
Vagina and uterus:
During the transition to menopause, menstrual patterns can show shorter cycling (by 2–7 days) longer cycles remain possible. There may be irregular bleeding (lighter, heavier, spotting). Dysfunctional uterine bleeding is often experienced by women approaching menopause due to the hormonal changes that accompany the menopause transition.
Spotting or bleeding may simply be related to vaginal atrophy, a benign sore (polyp or lesion), or may be a functional endometrial response. The European Menopause and Andropause Society has released guidelines for assessment of the endometrium, which is usually the main source of spotting or bleeding.
In post-menopausal women, however, any genital bleeding is an alarming symptom that requires an appropriate study to rule out the possibility of malignant diseases.
Symptoms that may appear during menopause and continue through postmenopause include:
Other physical symptoms:
Other physical symptoms of menopause include:
Mood and memory effects:
Psychological symptoms include anxiety, poor memory, inability to concentrate, depressive mood, irritability, mood swings, and less interest in sexual activity.
Menopause-related cognitive impairment can be confused with the mild cognitive impairment that precedes dementia. Forgetfulness affects about half of menopausal women, and is probably caused by the effects of declining estrogen levels on the brain, or perhaps by reduced blood flow to the brain during hot flashes.
Long-term effects:
Menopause confers:
Women who experience menopause before 45 years of age have an increased risk of heart disease, death, and impaired lung function.
Causes:
Menopause can be induced or occur naturally. Induced menopause occurs as a result of medical treatment such as:
Age:
Menopause typically occurs between 49 and 52 years of age. The majority of women have their last period between the ages of 48 and 55. The average age of the last period in the United States is 51 years, in the United Kingdom is 52 years, in Ireland is 50 years and in Australia is 51 years. In India and the Philippines, the median age of natural menopause is considerably earlier, at 44 years.
The menopausal transition or perimenopause leading up to menopause usually lasts 7 years (sometimes as long as 14 years).
In rare cases, a woman's ovaries stop working at a very early age, ranging anywhere from the age of puberty to age 40. This is known as premature ovarian failure and affects 1 to 2% of women by age 40.
Undiagnosed and untreated coeliac disease is a risk factor for early menopause. Coeliac disease can present with several non-gastrointestinal symptoms, in the absence of gastrointestinal symptoms, and most cases escape timely recognition and go undiagnosed, leading to a risk of long-term complications.
A strict gluten-free diet reduces the risk. Women with early diagnosis and treatment of coeliac disease present a normal duration of fertile life span.
Women who have undergone hysterectomy with ovary conservation go through menopause on average 3.7 years earlier than the expected age. Other factors that can promote an earlier onset of menopause (usually 1 to 3 years early) are smoking cigarettes or being extremely thin.
Premature ovarian failure:
Premature ovarian failure (POF) is the cessation of the ovarian function before the age of 40 years. It is diagnosed or confirmed by high blood levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH) on at least three occasions at least four weeks apart.
Known causes of premature ovarian failure include:
However, in about 50–80% of spontaneous cases of premature ovarian failure, the cause is unknown, i.e., it is generally idiopathic.
Women who have a functional disorder affecting the reproductive system (e.g., endometriosis, polycystic ovary syndrome, cancer of the reproductive organs) can go into menopause at a younger age than the normal timeframe. The functional disorders often significantly speed up the menopausal process.
An early menopause can be related to cigarette smoking, higher body mass index, racial and ethnic factors, illnesses, and the surgical removal of the ovaries, with or without the removal of the uterus.
Rates of premature menopause have been found to be significantly higher in fraternal and identical twins; approximately 5% of twins reach menopause before the age of 40. The reasons for this are not completely understood. Transplants of ovarian tissue between identical twins have been successful in restoring fertility.
Surgical menopause:
Menopause can be surgically induced by bilateral oophorectomy (removal of ovaries), which is often, but not always, done in conjunction with removal of the Fallopian tubes (salpingo-oophorectomy) and uterus (hysterectomy).
Cessation of menses as a result of removal of the ovaries is called "surgical menopause". Surgical treatments, such as the removal of ovaries, might cause periods to stop altogether. The sudden and complete drop in hormone levels usually produces extreme withdrawal symptoms such as hot flashes, etc. The symptoms of early menopause may be more severe.
Removal of the uterus without removal of the ovaries does not directly cause menopause, although pelvic surgery of this type can often precipitate a somewhat earlier menopause, perhaps because of a compromised blood supply to the ovaries. The time between surgery and possible early menopause is due to the fact that ovaries are still producing hormones.
Click on any of the following blue hyperlinks for more about Menopause:
Medical professionals often define menopause as having occurred when a woman has not had any vaginal bleeding for a year. It may also be defined by a decrease in hormone production by the ovaries.
In those who have had surgery to remove their uterus but still have ovaries, menopause may be considered to have occurred at the time of the surgery or when their hormone levels fell.
Following the removal of the uterus, symptoms typically occur earlier, at an average of 45 years of age.
In the years before menopause, a woman's periods typically become irregular, which means that periods may be longer or shorter in duration or be lighter or heavier in the amount of flow. During this time, women often experience hot flashes; these typically last from 30 seconds to ten minutes and may be associated with shivering, sweating, and reddening of the skin.
Hot flashes often stop occurring after a year or two. Other symptoms may include vaginal dryness, trouble sleeping, and mood changes. The severity of symptoms varies between women. While menopause is often thought to be linked to an increase in heart disease, this primarily occurs due to increasing age and does not have a direct relationship with menopause.
In some women, problems that were present like endometriosis or painful periods will improve after menopause.
Menopause is usually a natural change. It can occur earlier in those who smoke tobacco. Other causes include surgery that removes both ovaries or some types of chemotherapy.
At the physiological level, menopause happens because of a decrease in the ovaries' production of the hormones estrogen and progesterone.
While typically not needed, a diagnosis of menopause can be confirmed by measuring hormone levels in the blood or urine. Menopause is the opposite of menarche, the time when a girl's periods start.
Specific treatment is not usually needed. Some symptoms, however, may be improved with treatment. With respect to hot flashes, avoiding smoking, caffeine, and alcohol is often recommended. Sleeping in a cool room and using a fan may help. The following medications may help:
Exercise may help with sleeping problems.
While MHT was once routinely prescribed, it is now only recommended in those with significant symptoms, as there are concerns about side effects. High-quality evidence for the effectiveness of alternative medicine has not been found. There is tentative evidence for phytoestrogens.
Signs and symptoms:
During early menopause transition, the menstrual cycles remain regular but the interval between cycles begins to lengthen. Hormone levels begin to fluctuate. Ovulation may not occur with each cycle.
The date of the final menstrual period is usually taken as the point when menopause has occurred. During the menopausal transition and after menopause, women can experience a wide range of symptoms.
Vagina and uterus:
During the transition to menopause, menstrual patterns can show shorter cycling (by 2–7 days) longer cycles remain possible. There may be irregular bleeding (lighter, heavier, spotting). Dysfunctional uterine bleeding is often experienced by women approaching menopause due to the hormonal changes that accompany the menopause transition.
Spotting or bleeding may simply be related to vaginal atrophy, a benign sore (polyp or lesion), or may be a functional endometrial response. The European Menopause and Andropause Society has released guidelines for assessment of the endometrium, which is usually the main source of spotting or bleeding.
In post-menopausal women, however, any genital bleeding is an alarming symptom that requires an appropriate study to rule out the possibility of malignant diseases.
Symptoms that may appear during menopause and continue through postmenopause include:
- painful intercourse
- vaginal dryness
- atrophic vaginitis – thinning of the membranes of the vulva, the vagina, the cervix, and the outer urinary tract, along with considerable shrinking and loss in elasticity of all of the outer and inner genital areas.
Other physical symptoms:
Other physical symptoms of menopause include:
- lack of energy,
- joint soreness,
- stiffness,
- back pain,
- breast enlargement,
- breast pain,
- heart palpitations,
- headache,
- dizziness,
- dry, itchy skin,
- thinning,
- tingling skin,
- weight gain,
- urinary incontinence,
- urinary urgency,
- interrupted sleeping patterns,
- heavy night sweats,
- and hot flashes.
Mood and memory effects:
Psychological symptoms include anxiety, poor memory, inability to concentrate, depressive mood, irritability, mood swings, and less interest in sexual activity.
Menopause-related cognitive impairment can be confused with the mild cognitive impairment that precedes dementia. Forgetfulness affects about half of menopausal women, and is probably caused by the effects of declining estrogen levels on the brain, or perhaps by reduced blood flow to the brain during hot flashes.
Long-term effects:
Menopause confers:
- A possible but contentious increased risk of atherosclerosis. The risk of acute myocardial infarction and other cardiovascular diseases rises sharply after menopause, but the risk can be reduced by managing risk factors, such as tobacco smoking, hypertension, increased blood lipids and body weight.
- Increased risk of osteopenia, osteoporosis, and accelerated lung function decline.
Women who experience menopause before 45 years of age have an increased risk of heart disease, death, and impaired lung function.
Causes:
Menopause can be induced or occur naturally. Induced menopause occurs as a result of medical treatment such as:
- chemotherapy,
- radiotherapy,
- oophorectomy,
- or complications of tubal ligation,
- hysterectomy,
- unilateral or bilateral salpingo-oophorectomy
- or leuprorelin usage.
Age:
Menopause typically occurs between 49 and 52 years of age. The majority of women have their last period between the ages of 48 and 55. The average age of the last period in the United States is 51 years, in the United Kingdom is 52 years, in Ireland is 50 years and in Australia is 51 years. In India and the Philippines, the median age of natural menopause is considerably earlier, at 44 years.
The menopausal transition or perimenopause leading up to menopause usually lasts 7 years (sometimes as long as 14 years).
In rare cases, a woman's ovaries stop working at a very early age, ranging anywhere from the age of puberty to age 40. This is known as premature ovarian failure and affects 1 to 2% of women by age 40.
Undiagnosed and untreated coeliac disease is a risk factor for early menopause. Coeliac disease can present with several non-gastrointestinal symptoms, in the absence of gastrointestinal symptoms, and most cases escape timely recognition and go undiagnosed, leading to a risk of long-term complications.
A strict gluten-free diet reduces the risk. Women with early diagnosis and treatment of coeliac disease present a normal duration of fertile life span.
Women who have undergone hysterectomy with ovary conservation go through menopause on average 3.7 years earlier than the expected age. Other factors that can promote an earlier onset of menopause (usually 1 to 3 years early) are smoking cigarettes or being extremely thin.
Premature ovarian failure:
Premature ovarian failure (POF) is the cessation of the ovarian function before the age of 40 years. It is diagnosed or confirmed by high blood levels of follicle stimulating hormone (FSH) and luteinizing hormone (LH) on at least three occasions at least four weeks apart.
Known causes of premature ovarian failure include:
- autoimmune disorders,
- thyroid disease,
- diabetes mellitus,
- chemotherapy,
- being a carrier of the fragile X syndrome gene,
- and radiotherapy.
However, in about 50–80% of spontaneous cases of premature ovarian failure, the cause is unknown, i.e., it is generally idiopathic.
Women who have a functional disorder affecting the reproductive system (e.g., endometriosis, polycystic ovary syndrome, cancer of the reproductive organs) can go into menopause at a younger age than the normal timeframe. The functional disorders often significantly speed up the menopausal process.
An early menopause can be related to cigarette smoking, higher body mass index, racial and ethnic factors, illnesses, and the surgical removal of the ovaries, with or without the removal of the uterus.
Rates of premature menopause have been found to be significantly higher in fraternal and identical twins; approximately 5% of twins reach menopause before the age of 40. The reasons for this are not completely understood. Transplants of ovarian tissue between identical twins have been successful in restoring fertility.
Surgical menopause:
Menopause can be surgically induced by bilateral oophorectomy (removal of ovaries), which is often, but not always, done in conjunction with removal of the Fallopian tubes (salpingo-oophorectomy) and uterus (hysterectomy).
Cessation of menses as a result of removal of the ovaries is called "surgical menopause". Surgical treatments, such as the removal of ovaries, might cause periods to stop altogether. The sudden and complete drop in hormone levels usually produces extreme withdrawal symptoms such as hot flashes, etc. The symptoms of early menopause may be more severe.
Removal of the uterus without removal of the ovaries does not directly cause menopause, although pelvic surgery of this type can often precipitate a somewhat earlier menopause, perhaps because of a compromised blood supply to the ovaries. The time between surgery and possible early menopause is due to the fact that ovaries are still producing hormones.
Click on any of the following blue hyperlinks for more about Menopause:
Pornography, including in the United States
- YouTube Video: What Does Pornography Do to Your Brain?
- YouTube Video: A Day In The Life Of A Pornstar
- YouTube Video: EXCLUSIVE - Stormy Daniels Details Sex with Donald Trump
Pornography (often shortened to porn or porno) is the portrayal of sexual subject matter for the exclusive purpose of sexual arousal. A distinction could be drawn between uncensored explicit or hardcore erotic art, and pornography.
Pornography may be presented in a variety of media, including magazines, animation, writing, film, video, and video games. The term does not include live exhibitions like sex shows and striptease. The primary subjects of present-day pornographic depictions are pornographic models, who pose for still photographs, and pornographic actors who engage in filmed sex acts.
Various groups within society have considered depictions of a sexual nature immoral, addictive, and noxious, labeling them pornographic, and attempting to have them suppressed under obscenity laws, censored or made illegal. Such grounds, and even the definition of pornography, have differed in various historical, cultural, and national contexts.
In the late 19th century, various films by Thomas Edison were denounced as obscene in the United States, whereas Eugene Pirou's Le Coucher de la Mariée became very popular in France.
Social attitudes towards the discussion and presentation of sexuality have become more tolerant in Western countries, and legal definitions of obscenity have become more limited, beginning in 1969 with Blue Movie by Andy Warhol, the first adult erotic film depicting explicit sexual intercourse to receive wide theatrical release in the United States.
It was followed by the Golden Age of Porn (1969–1984), in which the best quality pornographic films became part of mainstream culture.
Top keywords searched online for pornography.A growing industry for the production and consumption of pornography developed in the latter half of the 20th century. The introduction of home video and the Internet saw a boom in the worldwide porn industry that generates billions of dollars annually.
Commercialized pornography accounts for over US$2.5 billion in the United States alone, including the production of various media and associated products and services.
The porn industry is between $10–$12 billion in the U.S. In 2006, the world pornography revenue was 97 billion dollars. This industry employs thousands of performers along with support and production staff. It is also followed by dedicated industry publications and trade groups, award shows such as the AVN Awards, as well as the mainstream press, private organizations (watchdog groups), government agencies, and political organizations.
Videos involving non-consensual content and cybersex trafficking have been hosted on popular pornography sites in the 21st century.
Click on any of the following blue hyperlinks for more about Pornography:
Pornography in the United States
Pornography in the United States has existed since the country's origins and has become more readily accessible in the 21st century. Advanced by technological development, it has gone from a hard-to-find "back alley" item, beginning in 1969 with Blue Movie by Andy Warhol, the Golden Age of Porn (1969–1984) and home video, to being more available in the country and later, starting in the 1990s, readily accessible to nearly anyone with a computer or other device connected to the Internet.
The U.S. has no current plans to block explicit content from children and adolescents, as many other countries have planned or proceeded to do.
Attempts made to suppress it include: outright bans, prohibitions of its sale, censorship or rating schemes that restrict audience numbers, and claims that it is prostitution and thereby subject to regulations governing prostitution.
Legal decisions affecting production and consumption of pornography include those relating to its definition, its relationship with prostitution, the definition of obscenity, rulings about personal possession of pornography, and its standing in relation to freedom of expression rights.
American advocates for pornography often cite the First Amendment to the United States Constitution, which guarantees freedom of speech; however, under the Miller test established by Miller v. California, anything lacking "serious literary, artistic, political, or scientific value" is generally not protected.
However, the Supreme Court of the United States held in Ashcroft v. Free Speech Coalition (2002) that pornography which involves consenting adults is protected by the First Amendment, even if the models "appear to be" minors but are, in fact of lawful age, and thus has seen to protect the majority of, but not all pornography on the basis of first-amendment law.
Publication:
Print:
American adult magazines which have the widest distribution do not violate the Miller test and can be legally distributed. Adult magazines have been largely put into mainstream by the pioneer Playboy. However, during the so-called Pubic Wars in the 1960s and 1970s Penthouse established itself as a more explicit magazine. Screw moved the bar toward hardcore when it first came out in 1968 and with Hustler appearing in 1974 the move to hardcore was complete.
By the mid-1990s magazines like Playboy had become noncompetitive and even hardcore publications like Penthouse and Hustler struggled.
According to Laura Kipnis, a cultural theorist and critic, "the Hustler body is an unromanticized body—no vaselined lens or soft focus: this is neither the airbrushed top-heavy fantasy body of Playboy, nor the ersatz opulence, the lingeried and sensitive crotch shots of Penthouse, transforming female genitals into objets d'art. It's a body, not a surface or a suntan: insistently material, defiantly vulgar, corporeal".
Many adult magazines in the United States are usually sold wrapped to avoid incidental viewing by minors and are now highlighted by special features or themes. For instance, a primarily softcore magazine, Barely Legal, focuses on models between 18 and 23 years of age. Hustler's Leg World is focused on the female legs and feet. Perfect 10 publishes images of women untouched by plastic surgery or airbrushing.
Pornographic bookstores have been subject to U.S. zoning laws.
Movies and pay-per-view:
See also: History of erotic depictions and Nudity in American television
Much of the pornography produced in the United States is in the form of movies and the branch acutely competes with the Internet. The market is very diverse and ranges from the mainstream heterosexual content to the rarefied S/M, BDSM, interracial sex, ethnic, etc. through enduringly popular gay porn.
Early American stag films included Wonders of the Unseen World (1927), An Author's True Story (1933), Goodyear (1950s), Smart Alec (1951), and Playmates (1956–58).
Breakthrough films, such as 1969's Blue Movie by Andy Warhol, 1972's Deep Throat, 1973's The Devil in Miss Jones and 1976's The Opening of Misty Beethoven by Radley Metzger, launched the so-called "porno chic" phenomenon in the United States and enabled the commercialization of the adult film industry.
In this period America's most notorious pornographer was Reuben Sturman. According to the U.S. Department of Justice, throughout the 1970s, Sturman controlled most of the pornography circulating in the country.
The country now houses over 40 adult movies studios featuring heterosexual scenes, more than any other country. The branch, according to founder and president of Adult Video News Paul Fishbein, involves the manufacturers of adult products, distributors, suppliers, retail store owners, wholesalers, distributors, cable TV buyers, and foreign buyers.
The production is concentrated in San Fernando Valley (mainly in Chatsworth, Reseda and Van Nuys) and Las Vegas, where more than 200 adult entertainment companies gather to network and show off their latest wares.
The world's largest adult movies studio, Vivid Entertainment, generates an estimated $100 million a year in revenue, distributing 60 films annually and selling them in video stores, hotel rooms, on cable systems, and on the Internet.
Vivid's two largest regional competitors are Wicked Pictures and Digital Playground. Boulder Colorado-based New Frontier Media, a leading distributor of adult movies (at NASDAQ since November 2000), is one of the two adult video companies traded publicly, the other one being Spanish Private Media Group.
The industry's decision to embrace VHS in the early 1980s, for example, helped to do away with Sony Betamax, despite the latter format's superior quality. Video rentals soared from just under 80 million in 1985 to half-billion by 1993. Suffering at the hands of video warez tended not be publicly stressed by country's film industry.
In 1999 there were 711 million rentals of hardcore films. 11,300 hardcore films were released in 2002.
In the recent years, according to Fishbein, there are well over 800 million rentals of adult videotapes and DVDs in video stores across the country. Digital Playground said it is choosing the Blu-ray Disc for all of its "interactive" films because of its greater capacity.
The female demographic is considered to be the biggest catalyst for pornographic cultural crossover. According to Adella O'Neal, a Digital Playground publicist, in 2000 roughly 9% of the company's consumers were women, while four years later that figure has bloomed to 53%.
American adult pay-per-view television is presently unregulated since it is not technically "broadcasting" as defined in the Federal Communications Act. Cable and satellite television networks host about six main adult-related channels.
Most of them (particularly Playboy TV, Penthouse TV, and Hustler TV (there is also a "Hustler Video", a line of raunchy films created by Larry Flynt)) are maintained by three mainstream porn magazines. In 1999 Playboy Enterprises sold to Vivid Entertainment a small channel which was renamed to Hot Network.
Since that Vivid launched two more channels—the Hot Zone and Vivid TV. The viewers paid close to $400 million a year to tune into Vivid's hardcore content and the company soon overtook Playboy as operator of the world's largest adult-TV network.
However, after passing the 2000 United States v. Playboy Entertainment Group case Playboy bought all three networks from Vivid in 2001 and folded them into "Playboy's Spice" brand. Operators then shunned "Playboy's Spice Platinum", a new group of channels with graphic hardcore fare.
Some subsidiaries of major corporations are the largest pornography sellers, like News Corporation's DirecTV. Comcast, the nation's largest cable company, once pulled in $50 million from adult programming. Revenues of companies such as Playboy and Hustler were small by comparison.
Video games and comics:
Microsoft has long declined to license development software to game makers whose titles include sexual content. Wal-Mart, America's largest distributor of video games, maintains the policy of selling no games with an AO rating.
However, in recent years the pornographic content in video games has been promoted particularly by Playboy. Playboy: The Mansion became the first game built around the "Playboy" license.
A downloadable mod—"Hot Coffee" for the game Grand Theft Auto: San Andreas brought attention to the need to discuss the challenges faced in creating games with pornographic content.
Meanwhile, Grand Theft Auto: San Andreas was pulled from shelves by Rockstar Games after it became public knowledge that, with the use of a Gameshark cheating device, the scene could be unlocked portraying the protagonist having sex with another character, although in the scene both characters have their clothes on. The game was later sold without the unlockable scene.
PlayStation 2 video game God of War (2005), based on Greek mythology, features an event in the first part of the game where protagonist Kratos can have sex with two topless prostitutes, who reside in a bedroom on his boat.
Although no sexual acts are depicted (they occur off-screen and are indicated by sound effects), the women are shown topless. The player interacts by performing button and joystick commands that appear on screen which results in an experience reward for the player.
This type of sex mini-game became a prominent feature for the God of War series, being included in its sequels God of War II (2007), God of War: Chains of Olympus (2008), God of War III (2010), and God of War: Ghost of Sparta (2010), with the latter being the final game to feature it.
The adult sections of American comic book stores frequently carry a large number of translations of Japanese hardcore comics, as well as an increasing number of home imitations.
One of the Japanese animation porn movies, which started the American adult video market, was Urotsukidoji. The adult animation market exists primarily through direct sales: mail-order to customers, and wholesale to specialty shops which cater to animation and to comic-book fans.
The legal framework in both countries regarding the regulation of obscene and pornographic material is overall rather similar.
Internet:
The Internet maintains a significant part of American adult entertainment, also because the 1997 Reno v. American Civil Liberties Union case specified that the term "indecent" has no specific legal meaning in the context of the Internet.
More recent federal efforts, such as the CAN-SPAM Act of 2003 expressly addressed the Internet. On May 1, 2000, American Express announced it would no longer cover transactions from adult sites.
According to the committee to Study Tools and Strategies for Protecting Kids from Pornography and Their Applicability to Other Inappropriate Internet Content, there are over 100,000 subscription sites with adult content in the United States, with each site having multiple web pages.
On average, a paid subscription generates $20 to $40 per month in revenue, however, an in-depth analysis is complicated. If a visitor site connects to a pay site and signs up for content, it receives a conversion fee from the larger site. A successful large operation is often an umbrella company serving many markets with pay sites. Around this core and its affiliates is a system of ad-supported service sites. The so-called portable porn market is in its initial stage in the U.S.
In 2000 the owners and operators of Playgirl.com and scores of other adult sites were charged by the U.S. Federal Trade Commission with illegally billing thousands of consumers for services that were advertised as free, and for billing other consumers who never visited the web sites at all.
Nevadan Voice Media Incorporated, which ran several adult sites, was also charged by the commission. Sites often suffer from unauthorized, non-paying surfers who use stolen passwords, which can use a month's worth of bandwidth in a day, costing the site operator hundreds or thousands of dollars' worth of additional bandwidth fees, all for traffic that returns no money at all.
The 2002 Paragon Electric Co., Inc. v. Buy This Domain case ruled that linking domain names to pornographic sites is not per se conclusive of bad-faith registration and use, although it does raise that presumption.
A common occurrence was the use of domain names similar to known ones, such as whitehouse.com (unrelated to whitehouse.gov), which for some period featured explicit content. The use of expired domains is also common, along with typosquatting, which relies on mistakes such as typos made by Internet users when inputting a website address into a web browser.
Economics:
In 1975, the total retail value of all the hardcore pornography in the U.S. was estimated at $5–10 million. The 1979 Revision of the Federal Criminal Code stated that "in Los Angeles alone, the pornography business does $100 million a year in gross retail volume" while "the average pornography magazine sells for between $6 and $10 each".
According to the 1986 Attorney General's Commission on Pornography, American adult entertainment industry has grown considerably over the past thirty years by continually changing and expanding to appeal to new markets, though the production is considered to be low-profile and clandestine.
The total income of modern country's adult entertainment is often rated at $10–13 billion, of which $4–6 billion are legal. The figure is often credited to a study by Forrester Research and was lowered in 1998. In 2007 The Observer newspaper also gave a figure of $13 billion.
Other sources, quoted by Forbes (Adams Media Research, Veronis Suhler Communications Industry Report, and IVD), even taking into consideration all possible means (video networks and pay-per-view movies on cable and satellite, web sites, in-room hotel movies, phone sex, sex toys, and magazines) mention the $2.6–3.9 billion figure (without the cellphone component).
USA Today claimed in 2003 that websites such as Danni's Hard Drive and Cybererotica.com generated $2 billion in revenue in that year, which was allegedly about 10% of the overall domestic porn market at the time. The adult movies income (from sale and rent) was once estimated by AVN Publications at $4.3 billion but how this figure was determined is unclear. According to the 2001 Forbes data the annual income distribution is like this:
Adult Video: $500 million to $1.8 billion:
AS: Internet: $1 billion
Magazines: $1 billion
Pay-per-view: $128 Million
Cellphones: $ 30 Million
The Online Journalism Review, published by the Annenberg School of Communication at the University of Southern California, weighed in with an analysis that favored Forbes' number.
The financial extent of adult films, distributed in hotels, is hard to estimate—hotels keep statistics to themselves or do not keep them at all. A CBS News investigation in November 2003 claimed that 50% of guests at the Hilton, Marriott, Hyatt, Sheraton, and Holiday Inn hotel chains purchased adult movies, contributing to 70% of in-room profits.
The income of cellphone porn is low, when compared with other countries. The absence of V-chip-style parental controls on other equipment has obviated the need for American consumers to use cellphones to access explicit content.
Legality:
Further information: See also
The lawful definition of pornography in the U.S. evolved through decades, from the 1960s. In this period, recognizing ambiguities, the term "sexually explicit content" gained use as one of the pornography's euphemisms, but later it was determined that a distinction between pornographic and sexually explicit content is completely artificial.
In Miller v. California the Supreme Court used the definition of pornography made by Webster's Third New International Dictionary of 1969 ("a depiction (as in a writing or painting) of licentiousness or lewdness: a portrayal of erotic behavior designed to cause sexual excitement").
Black's Law Dictionary followed the Miller test and defined pornography as material that taken as a whole the average person, applying contemporary community standards, would find appealing to the prurient interest.
Heinle's Newbury House Dictionary of American English (2003) defined pornography as "obscene writings, pictures, or films intended to arouse sexual desire".
The Antipornography Civil Rights Ordinance defined pornography as the "graphic sexually explicit subordination of women, whether in pictures or in words". The ordinance was ruled unconstitutional by the Federal Appeals Court in American Booksellers v. Hudnut in Indianapolis (1985).
Courts in California and New York have clearly rejected the argument that the making of pornography is prostitution. (See California v. Freeman (1988) and People v. Paulino (2005).)
The Oregon Supreme Court went even further in State v. Henry (1987) by abolishing the legal definition of obscenity in that state, ruling it violated freedom of speech as defined in the state constitution.
Pornography as a legal term at the federal level, except the generic terms "hardcore pornography" and "child pornography", has not existed since the 1973 Miller v. California case.
The United States Supreme Court in Miller v. California discussed pornography (which it referred to as "sexually explicit material") in terms of obscenity, which it held did not enjoy First Constitutional Amendment protection, but recognized that individual communities had different values and opinions on obscenity.
The Court's definition of obscenity has come to be called the Miller test. Since then several States have passed laws in terms of that test.
Relying on the 1930 Smoot–Hawley Tariff Act and under the terms "obscene" and "immoral", the U.S. Customs and Border Protection prohibits the importation of any pornographic material (19 U.S.C. "Immoral articles; importation prohibited").
Pornography as prostitution:
Attempts were made in the United States in the 1970s to close down the pornography industry by prosecuting those in the industry on prostitution charges. The prosecution started in the courts in California in the case of People v. Freeman.
The California Supreme Court acquitted Freeman and distinguished between someone who takes part in a sexual relationship for money (prostitution) versus someone whose role is merely portraying a sexual relationship on-screen as part of their acting performance.
The State did not appeal to the United States Supreme Court making the decision binding in California, where most pornographic films are made today.
Origin of term:
The term "pornography" first appeared in an 1857 British medical dictionary, which defined it as "a description of prostitutes or of prostitution, as a matter of public hygiene", therefore pornography by itself was not a widely used term in nineteenth-century America and the term did not appear in any version of American Dictionary of the English Language in its early editions.
The dictionary introduced the entry in 1864, defining it primarily as a "treatment of, or a treatise on, the subject of prostitutes or prostitution". Early charges used the term "obscenity" as well as after Miller v. California, though the term "pornography" remained as a reference entry:
The censorship of pornographic materials in the United States was enabled by the way courts interpreted the First, and partially Ninth and Fourteenth amendments to the U.S. Constitution.
The legal justification also includes the so-called harm principle, as in Canada and the United Kingdom. The absolutist interpretation of the First Amendment as applied to pornography has never been sustained by the Supreme Court.
In the Investigation of Literature Allegedly Containing Objectionable Material, issued by the U.S. Congress Select Committee on Current Pornographic Materials in 1953, it was noted that "perhaps the greatest impediments to the prompt and effective enforcement of existing laws intended to control pornographic materials are the difficulties of establishing a precise interpretation of the word".
During the Warren Court (1953–1969), the first notable court to face the cases of such kind, justices Potter Stewart, Byron White, and Arthur Goldberg shared the opinion that only hardcore pornography was not protected by the First and Fourteenth Amendments. This position was contested notably by U.S. Solicitor General James Lee Rankin (in office 1956–1961), but in Jacobellis v. Ohio Stewart concluded that criminal obscenity laws are constitutionally limited under the First and Fourteenth Amendments to hardcore pornography.
Concurring in the 1957 Roth v. United States Justice John Marshall Harlan II wrote that "even assuming that pornography cannot be deemed ever to cause, in an immediate sense, criminal sexual conduct, other interests within the proper cognizance of the States may be protected by the prohibition placed on such materials."
The 1967 Public Law 90-100 found the traffic in pornography to be "a matter of national concern", as well as in obscenity. In this period the Court considered pornography to have two major dimensions:
A frustration was expressed notably by Justice Hugo Black in the 1966 Mishkin v. New York: "I wish once more to express my objections to saddling this Court with the irksome and inevitably unpopular and unwholesome task of finally deciding by a case-by-case, sight-by-sight personal judgment of the members of this Court what pornography (whatever that means) is too hard core for people to see or read."
In the 1974 Hamling v. United States decision the Supreme Court said that just because pornographic materials are for sale and purchased around the country, "Mere availability of similar materials by itself means nothing more than that other persons are engaged in similar activities."
The 1976 American Heritage Dictionary of the English Language defined that pornography consists of "written, graphic, or other forms of communication intended to excite lascivious feelings". Since determining what is pornography and what is "soft core" and "hard core" are subjective questions to judges, juries, and law enforcement officials, it is difficult to define, since the law cases cannot print examples for the courts to follow.
The Rehnquist Court further enhanced the power of community controls on pornography. Current Chief Justice John Roberts told at the confirmation hearing on his nomination: "Well, Senator, it's my understanding under the Supreme Court's doctrine that pornographic expression is not protected to the same extent at least as political and core speech, and the difficulty that the Court has addressed in these different areas of course is always defining what is or is not pornography and what is entitled to protection under the First Amendment and what is not".
The famous Indianapolis definition of pornography by Dworkin and MacKinnon paralleled their Minneapolis ordinance. The first was rejected by the United States Court of Appeals for the Seventh Circuit for several reasons. The ordinance did not use any of the accepted terms that the Supreme Court had developed over time for determining when material is obscene, including "prurient interest", "offensiveness", or "local community standards".
Another concern was the way the women were depicted in the work. If women were referred to in the approved fashion stressing equality, the activity involved would be regardless of how sexually explicit it was.The Court also indicated that if women were referred to in a disapproving way depicting them as subversive or as enjoying humiliation, the activity would be unlawful regardless of the "literary, artistic or political qualities of the work taken as a whole".
Judge Frank Easterbrook said: "We accept the premises of this legislation. Depictions of subordination tend to perpetuate subordination. The subordinate status of women in turn leads to affront and lower pay at work, insult and injury at home, battery and rape on the streets.... Yet this simply demonstrates the power of pornography as speech."
Conceptions of Democracy in American Constitutional Argument: The Case of Pornography Regulation by Frank Michelman, issued by Tennessee Law Review (vol. 56, no. 291, 1989) partially consented that "pornography is political expression in that it promulgates a certain view of women's natures and thus of women's appropriate relations and treatment in society", but also concluded that the Indianapolis ordinance was precisely designed to suppress that particular view by censoring pornography.
Minneapolis ordinance was struck down on the grounds that it was ambiguous and vague, however, despite of its failure the proposal influenced other communities across the United States.
In May 2005 U.S. Attorney General Alberto Gonzales established an Obscenity Prosecution Task Force. The task force, according to a Department of Justice news release on May 5, was "dedicated to the investigation and prosecution of the distributors of hard-core pornography that meets the test for obscenity, as defined by the United States Supreme Court."
Under President Bush's and Gonzales' rationales the FBI Adult Obscenity Squad was recruited in August 2005 to gather evidence against "manufacturers and purveyors" of adult pornography.
Child pornography:
Main articles:
The 1970 Lockhart Commission recommended eliminating all criminal penalties for pornography except for pornographic depictions of minors, or sale of pornography to minors.
However, prior to 1977, only two states had laws which prohibited the use of children in the production or distribution of pornographic materials or performances.
In 1977, the Department of Justice strongly endorsed legislation which banned the production and dissemination of child pornography. These efforts have been unsuccessfully challenged in the 1982 New York v. Ferber case ("The States are entitled to greater leeway in the regulation of pornographic depictions of children...").
Although the states have a different age of consent, in accordance with the Federal Labeling and Record-Keeping Law all models featured in pornographic content should be at least 18 years of age. This kind of material is often labeled as "adult" and the appropriate disclaimers are common.
They are based on what "depicts or describes, in terms patently offensive as measured by contemporary community standards, sexual or excretory activities or organs".
It is a federal crime to possess, distribute, or produce non-fictional child pornography and carries large fines and prison sentences of up to 30 years upon conviction and requirement to register as a sex offender.
Anti-pornography movement:
Main article: Anti-pornography movement in the United States
An anti-pornography movement has existed in the United States since before the 1969 Supreme Court decision of Stanley v. Georgia, which held that people could view whatever they wished in the privacy of their own homes, by establishing an implied "right to privacy" in U.S. law. This led President Lyndon B. Johnson, with the backing of Congress, to appoint a commission to study pornography.
The anti-pornography movement seeks to maintain or restore restrictions and to increase or create restrictions on the production, sale or dissemination of pornography.
Jesuit priest Father Morton A. Hill (1917-1985) was a leader of the campaign against pornography in the United States in the 1960s, 1970s and 1980s. He was one of the founders of Morality in Media, which was created in 1962 to fight pornography.
Morality in Media was launched by an interfaith group of clergy and Hill was president until his death in 1985. Morality in Media continues with Patrick A. Trueman, a registered federal lobbyist, as president.
So prominent was Hill on the issue, that in 1969 President Lyndon B. Johnson appointed him to the President's Commission on Obscenity and Pornography. Father Hill and another clergyman on the commission, Dr. Winfrey C. Link, believed that the commission was stacked with supporters of loosening laws on pornography, and issued the Hill-Link Minority Report rebutting the conclusions of the majority report, which held that pornography should be decriminalized as there were no links between it and criminal behavior.
The majority report was widely criticized and rejected by Congress. The Senate rejected the commission's findings and recommendations by a 60–5 vote, with 34 abstentions. President Nixon, who had succeeded Johnson in 1969, also emphatically rejected the majority report.
The Hill-Link Minority Report, on the other hand, which recommended maintaining anti-obscenity statutes, was read into the record of both the United States Senate and the United States House of Representatives. It was cited by the Burger Court in its 1973 obscenity decisions, including Miller v. California.
See also:
Pornography may be presented in a variety of media, including magazines, animation, writing, film, video, and video games. The term does not include live exhibitions like sex shows and striptease. The primary subjects of present-day pornographic depictions are pornographic models, who pose for still photographs, and pornographic actors who engage in filmed sex acts.
Various groups within society have considered depictions of a sexual nature immoral, addictive, and noxious, labeling them pornographic, and attempting to have them suppressed under obscenity laws, censored or made illegal. Such grounds, and even the definition of pornography, have differed in various historical, cultural, and national contexts.
In the late 19th century, various films by Thomas Edison were denounced as obscene in the United States, whereas Eugene Pirou's Le Coucher de la Mariée became very popular in France.
Social attitudes towards the discussion and presentation of sexuality have become more tolerant in Western countries, and legal definitions of obscenity have become more limited, beginning in 1969 with Blue Movie by Andy Warhol, the first adult erotic film depicting explicit sexual intercourse to receive wide theatrical release in the United States.
It was followed by the Golden Age of Porn (1969–1984), in which the best quality pornographic films became part of mainstream culture.
Top keywords searched online for pornography.A growing industry for the production and consumption of pornography developed in the latter half of the 20th century. The introduction of home video and the Internet saw a boom in the worldwide porn industry that generates billions of dollars annually.
Commercialized pornography accounts for over US$2.5 billion in the United States alone, including the production of various media and associated products and services.
The porn industry is between $10–$12 billion in the U.S. In 2006, the world pornography revenue was 97 billion dollars. This industry employs thousands of performers along with support and production staff. It is also followed by dedicated industry publications and trade groups, award shows such as the AVN Awards, as well as the mainstream press, private organizations (watchdog groups), government agencies, and political organizations.
Videos involving non-consensual content and cybersex trafficking have been hosted on popular pornography sites in the 21st century.
Click on any of the following blue hyperlinks for more about Pornography:
- Etymology
- History
- Classification
- Commercialism
- Viewing effects
- Laws and regulations
- STI prevention and birth control methods
- Views
- See also:
- Effects of pornography on relationships
- Erotic literature
- Erotic photography
- Sex in advertising
- Sex-positive feminism
- Sex worker
- Commentary
- "American Porn". Frontline. PBS. Retrieved 1 February 2014. Interactive web site companion to a Frontline documentary exploring the pornography industry within the United States.
- Economics
- Susannah Breslin (20 December 2013). "LEADERSHIP: What Porn Stars Do When The Porn Industry Shuts Down". Forbes.
- Government
- Kutchinsky, Berl, Professor of Criminology: The first law that legalized pornography (Denmark)
- History
- Patricia Davis, PhD, Simon Noble & Rebecca J. White (2010). The History of Modern Pornography. History.com.
- Law
- Sociology
- Diamond, M. and Uchiyama, A. (1999). "Pornography, Rape and Sex Crimes in Japan". International Journal of Law and Psychiatry.
- West, Caroline (5 May 2004). "Pornography and Censorship". Stanford Encyclopedia of Philosophy.
- Technology
Pornography in the United States
Pornography in the United States has existed since the country's origins and has become more readily accessible in the 21st century. Advanced by technological development, it has gone from a hard-to-find "back alley" item, beginning in 1969 with Blue Movie by Andy Warhol, the Golden Age of Porn (1969–1984) and home video, to being more available in the country and later, starting in the 1990s, readily accessible to nearly anyone with a computer or other device connected to the Internet.
The U.S. has no current plans to block explicit content from children and adolescents, as many other countries have planned or proceeded to do.
Attempts made to suppress it include: outright bans, prohibitions of its sale, censorship or rating schemes that restrict audience numbers, and claims that it is prostitution and thereby subject to regulations governing prostitution.
Legal decisions affecting production and consumption of pornography include those relating to its definition, its relationship with prostitution, the definition of obscenity, rulings about personal possession of pornography, and its standing in relation to freedom of expression rights.
American advocates for pornography often cite the First Amendment to the United States Constitution, which guarantees freedom of speech; however, under the Miller test established by Miller v. California, anything lacking "serious literary, artistic, political, or scientific value" is generally not protected.
However, the Supreme Court of the United States held in Ashcroft v. Free Speech Coalition (2002) that pornography which involves consenting adults is protected by the First Amendment, even if the models "appear to be" minors but are, in fact of lawful age, and thus has seen to protect the majority of, but not all pornography on the basis of first-amendment law.
Publication:
Print:
American adult magazines which have the widest distribution do not violate the Miller test and can be legally distributed. Adult magazines have been largely put into mainstream by the pioneer Playboy. However, during the so-called Pubic Wars in the 1960s and 1970s Penthouse established itself as a more explicit magazine. Screw moved the bar toward hardcore when it first came out in 1968 and with Hustler appearing in 1974 the move to hardcore was complete.
By the mid-1990s magazines like Playboy had become noncompetitive and even hardcore publications like Penthouse and Hustler struggled.
According to Laura Kipnis, a cultural theorist and critic, "the Hustler body is an unromanticized body—no vaselined lens or soft focus: this is neither the airbrushed top-heavy fantasy body of Playboy, nor the ersatz opulence, the lingeried and sensitive crotch shots of Penthouse, transforming female genitals into objets d'art. It's a body, not a surface or a suntan: insistently material, defiantly vulgar, corporeal".
Many adult magazines in the United States are usually sold wrapped to avoid incidental viewing by minors and are now highlighted by special features or themes. For instance, a primarily softcore magazine, Barely Legal, focuses on models between 18 and 23 years of age. Hustler's Leg World is focused on the female legs and feet. Perfect 10 publishes images of women untouched by plastic surgery or airbrushing.
Pornographic bookstores have been subject to U.S. zoning laws.
Movies and pay-per-view:
See also: History of erotic depictions and Nudity in American television
Much of the pornography produced in the United States is in the form of movies and the branch acutely competes with the Internet. The market is very diverse and ranges from the mainstream heterosexual content to the rarefied S/M, BDSM, interracial sex, ethnic, etc. through enduringly popular gay porn.
Early American stag films included Wonders of the Unseen World (1927), An Author's True Story (1933), Goodyear (1950s), Smart Alec (1951), and Playmates (1956–58).
Breakthrough films, such as 1969's Blue Movie by Andy Warhol, 1972's Deep Throat, 1973's The Devil in Miss Jones and 1976's The Opening of Misty Beethoven by Radley Metzger, launched the so-called "porno chic" phenomenon in the United States and enabled the commercialization of the adult film industry.
In this period America's most notorious pornographer was Reuben Sturman. According to the U.S. Department of Justice, throughout the 1970s, Sturman controlled most of the pornography circulating in the country.
The country now houses over 40 adult movies studios featuring heterosexual scenes, more than any other country. The branch, according to founder and president of Adult Video News Paul Fishbein, involves the manufacturers of adult products, distributors, suppliers, retail store owners, wholesalers, distributors, cable TV buyers, and foreign buyers.
The production is concentrated in San Fernando Valley (mainly in Chatsworth, Reseda and Van Nuys) and Las Vegas, where more than 200 adult entertainment companies gather to network and show off their latest wares.
The world's largest adult movies studio, Vivid Entertainment, generates an estimated $100 million a year in revenue, distributing 60 films annually and selling them in video stores, hotel rooms, on cable systems, and on the Internet.
Vivid's two largest regional competitors are Wicked Pictures and Digital Playground. Boulder Colorado-based New Frontier Media, a leading distributor of adult movies (at NASDAQ since November 2000), is one of the two adult video companies traded publicly, the other one being Spanish Private Media Group.
The industry's decision to embrace VHS in the early 1980s, for example, helped to do away with Sony Betamax, despite the latter format's superior quality. Video rentals soared from just under 80 million in 1985 to half-billion by 1993. Suffering at the hands of video warez tended not be publicly stressed by country's film industry.
In 1999 there were 711 million rentals of hardcore films. 11,300 hardcore films were released in 2002.
In the recent years, according to Fishbein, there are well over 800 million rentals of adult videotapes and DVDs in video stores across the country. Digital Playground said it is choosing the Blu-ray Disc for all of its "interactive" films because of its greater capacity.
The female demographic is considered to be the biggest catalyst for pornographic cultural crossover. According to Adella O'Neal, a Digital Playground publicist, in 2000 roughly 9% of the company's consumers were women, while four years later that figure has bloomed to 53%.
American adult pay-per-view television is presently unregulated since it is not technically "broadcasting" as defined in the Federal Communications Act. Cable and satellite television networks host about six main adult-related channels.
Most of them (particularly Playboy TV, Penthouse TV, and Hustler TV (there is also a "Hustler Video", a line of raunchy films created by Larry Flynt)) are maintained by three mainstream porn magazines. In 1999 Playboy Enterprises sold to Vivid Entertainment a small channel which was renamed to Hot Network.
Since that Vivid launched two more channels—the Hot Zone and Vivid TV. The viewers paid close to $400 million a year to tune into Vivid's hardcore content and the company soon overtook Playboy as operator of the world's largest adult-TV network.
However, after passing the 2000 United States v. Playboy Entertainment Group case Playboy bought all three networks from Vivid in 2001 and folded them into "Playboy's Spice" brand. Operators then shunned "Playboy's Spice Platinum", a new group of channels with graphic hardcore fare.
Some subsidiaries of major corporations are the largest pornography sellers, like News Corporation's DirecTV. Comcast, the nation's largest cable company, once pulled in $50 million from adult programming. Revenues of companies such as Playboy and Hustler were small by comparison.
Video games and comics:
Microsoft has long declined to license development software to game makers whose titles include sexual content. Wal-Mart, America's largest distributor of video games, maintains the policy of selling no games with an AO rating.
However, in recent years the pornographic content in video games has been promoted particularly by Playboy. Playboy: The Mansion became the first game built around the "Playboy" license.
A downloadable mod—"Hot Coffee" for the game Grand Theft Auto: San Andreas brought attention to the need to discuss the challenges faced in creating games with pornographic content.
Meanwhile, Grand Theft Auto: San Andreas was pulled from shelves by Rockstar Games after it became public knowledge that, with the use of a Gameshark cheating device, the scene could be unlocked portraying the protagonist having sex with another character, although in the scene both characters have their clothes on. The game was later sold without the unlockable scene.
PlayStation 2 video game God of War (2005), based on Greek mythology, features an event in the first part of the game where protagonist Kratos can have sex with two topless prostitutes, who reside in a bedroom on his boat.
Although no sexual acts are depicted (they occur off-screen and are indicated by sound effects), the women are shown topless. The player interacts by performing button and joystick commands that appear on screen which results in an experience reward for the player.
This type of sex mini-game became a prominent feature for the God of War series, being included in its sequels God of War II (2007), God of War: Chains of Olympus (2008), God of War III (2010), and God of War: Ghost of Sparta (2010), with the latter being the final game to feature it.
The adult sections of American comic book stores frequently carry a large number of translations of Japanese hardcore comics, as well as an increasing number of home imitations.
One of the Japanese animation porn movies, which started the American adult video market, was Urotsukidoji. The adult animation market exists primarily through direct sales: mail-order to customers, and wholesale to specialty shops which cater to animation and to comic-book fans.
The legal framework in both countries regarding the regulation of obscene and pornographic material is overall rather similar.
Internet:
The Internet maintains a significant part of American adult entertainment, also because the 1997 Reno v. American Civil Liberties Union case specified that the term "indecent" has no specific legal meaning in the context of the Internet.
More recent federal efforts, such as the CAN-SPAM Act of 2003 expressly addressed the Internet. On May 1, 2000, American Express announced it would no longer cover transactions from adult sites.
According to the committee to Study Tools and Strategies for Protecting Kids from Pornography and Their Applicability to Other Inappropriate Internet Content, there are over 100,000 subscription sites with adult content in the United States, with each site having multiple web pages.
On average, a paid subscription generates $20 to $40 per month in revenue, however, an in-depth analysis is complicated. If a visitor site connects to a pay site and signs up for content, it receives a conversion fee from the larger site. A successful large operation is often an umbrella company serving many markets with pay sites. Around this core and its affiliates is a system of ad-supported service sites. The so-called portable porn market is in its initial stage in the U.S.
In 2000 the owners and operators of Playgirl.com and scores of other adult sites were charged by the U.S. Federal Trade Commission with illegally billing thousands of consumers for services that were advertised as free, and for billing other consumers who never visited the web sites at all.
Nevadan Voice Media Incorporated, which ran several adult sites, was also charged by the commission. Sites often suffer from unauthorized, non-paying surfers who use stolen passwords, which can use a month's worth of bandwidth in a day, costing the site operator hundreds or thousands of dollars' worth of additional bandwidth fees, all for traffic that returns no money at all.
The 2002 Paragon Electric Co., Inc. v. Buy This Domain case ruled that linking domain names to pornographic sites is not per se conclusive of bad-faith registration and use, although it does raise that presumption.
A common occurrence was the use of domain names similar to known ones, such as whitehouse.com (unrelated to whitehouse.gov), which for some period featured explicit content. The use of expired domains is also common, along with typosquatting, which relies on mistakes such as typos made by Internet users when inputting a website address into a web browser.
Economics:
In 1975, the total retail value of all the hardcore pornography in the U.S. was estimated at $5–10 million. The 1979 Revision of the Federal Criminal Code stated that "in Los Angeles alone, the pornography business does $100 million a year in gross retail volume" while "the average pornography magazine sells for between $6 and $10 each".
According to the 1986 Attorney General's Commission on Pornography, American adult entertainment industry has grown considerably over the past thirty years by continually changing and expanding to appeal to new markets, though the production is considered to be low-profile and clandestine.
The total income of modern country's adult entertainment is often rated at $10–13 billion, of which $4–6 billion are legal. The figure is often credited to a study by Forrester Research and was lowered in 1998. In 2007 The Observer newspaper also gave a figure of $13 billion.
Other sources, quoted by Forbes (Adams Media Research, Veronis Suhler Communications Industry Report, and IVD), even taking into consideration all possible means (video networks and pay-per-view movies on cable and satellite, web sites, in-room hotel movies, phone sex, sex toys, and magazines) mention the $2.6–3.9 billion figure (without the cellphone component).
USA Today claimed in 2003 that websites such as Danni's Hard Drive and Cybererotica.com generated $2 billion in revenue in that year, which was allegedly about 10% of the overall domestic porn market at the time. The adult movies income (from sale and rent) was once estimated by AVN Publications at $4.3 billion but how this figure was determined is unclear. According to the 2001 Forbes data the annual income distribution is like this:
Adult Video: $500 million to $1.8 billion:
AS: Internet: $1 billion
Magazines: $1 billion
Pay-per-view: $128 Million
Cellphones: $ 30 Million
The Online Journalism Review, published by the Annenberg School of Communication at the University of Southern California, weighed in with an analysis that favored Forbes' number.
The financial extent of adult films, distributed in hotels, is hard to estimate—hotels keep statistics to themselves or do not keep them at all. A CBS News investigation in November 2003 claimed that 50% of guests at the Hilton, Marriott, Hyatt, Sheraton, and Holiday Inn hotel chains purchased adult movies, contributing to 70% of in-room profits.
The income of cellphone porn is low, when compared with other countries. The absence of V-chip-style parental controls on other equipment has obviated the need for American consumers to use cellphones to access explicit content.
Legality:
Further information: See also
The lawful definition of pornography in the U.S. evolved through decades, from the 1960s. In this period, recognizing ambiguities, the term "sexually explicit content" gained use as one of the pornography's euphemisms, but later it was determined that a distinction between pornographic and sexually explicit content is completely artificial.
In Miller v. California the Supreme Court used the definition of pornography made by Webster's Third New International Dictionary of 1969 ("a depiction (as in a writing or painting) of licentiousness or lewdness: a portrayal of erotic behavior designed to cause sexual excitement").
Black's Law Dictionary followed the Miller test and defined pornography as material that taken as a whole the average person, applying contemporary community standards, would find appealing to the prurient interest.
Heinle's Newbury House Dictionary of American English (2003) defined pornography as "obscene writings, pictures, or films intended to arouse sexual desire".
The Antipornography Civil Rights Ordinance defined pornography as the "graphic sexually explicit subordination of women, whether in pictures or in words". The ordinance was ruled unconstitutional by the Federal Appeals Court in American Booksellers v. Hudnut in Indianapolis (1985).
Courts in California and New York have clearly rejected the argument that the making of pornography is prostitution. (See California v. Freeman (1988) and People v. Paulino (2005).)
The Oregon Supreme Court went even further in State v. Henry (1987) by abolishing the legal definition of obscenity in that state, ruling it violated freedom of speech as defined in the state constitution.
Pornography as a legal term at the federal level, except the generic terms "hardcore pornography" and "child pornography", has not existed since the 1973 Miller v. California case.
The United States Supreme Court in Miller v. California discussed pornography (which it referred to as "sexually explicit material") in terms of obscenity, which it held did not enjoy First Constitutional Amendment protection, but recognized that individual communities had different values and opinions on obscenity.
The Court's definition of obscenity has come to be called the Miller test. Since then several States have passed laws in terms of that test.
Relying on the 1930 Smoot–Hawley Tariff Act and under the terms "obscene" and "immoral", the U.S. Customs and Border Protection prohibits the importation of any pornographic material (19 U.S.C. "Immoral articles; importation prohibited").
Pornography as prostitution:
Attempts were made in the United States in the 1970s to close down the pornography industry by prosecuting those in the industry on prostitution charges. The prosecution started in the courts in California in the case of People v. Freeman.
The California Supreme Court acquitted Freeman and distinguished between someone who takes part in a sexual relationship for money (prostitution) versus someone whose role is merely portraying a sexual relationship on-screen as part of their acting performance.
The State did not appeal to the United States Supreme Court making the decision binding in California, where most pornographic films are made today.
Origin of term:
The term "pornography" first appeared in an 1857 British medical dictionary, which defined it as "a description of prostitutes or of prostitution, as a matter of public hygiene", therefore pornography by itself was not a widely used term in nineteenth-century America and the term did not appear in any version of American Dictionary of the English Language in its early editions.
The dictionary introduced the entry in 1864, defining it primarily as a "treatment of, or a treatise on, the subject of prostitutes or prostitution". Early charges used the term "obscenity" as well as after Miller v. California, though the term "pornography" remained as a reference entry:
- Merriam-Webster's Dictionary of Law": Material that depicts erotic behavior and is intended to cause sexual excitement"
- West's Encyclopedia of American Law": The representation in books, magazines, photographs, films, and other media of scenes of sexual behavior that are erotic or lewd and are designed to arouse sexual interest"; "the depiction of sexual behavior that is intended to arouse sexual excitement in its audience"
The censorship of pornographic materials in the United States was enabled by the way courts interpreted the First, and partially Ninth and Fourteenth amendments to the U.S. Constitution.
The legal justification also includes the so-called harm principle, as in Canada and the United Kingdom. The absolutist interpretation of the First Amendment as applied to pornography has never been sustained by the Supreme Court.
In the Investigation of Literature Allegedly Containing Objectionable Material, issued by the U.S. Congress Select Committee on Current Pornographic Materials in 1953, it was noted that "perhaps the greatest impediments to the prompt and effective enforcement of existing laws intended to control pornographic materials are the difficulties of establishing a precise interpretation of the word".
During the Warren Court (1953–1969), the first notable court to face the cases of such kind, justices Potter Stewart, Byron White, and Arthur Goldberg shared the opinion that only hardcore pornography was not protected by the First and Fourteenth Amendments. This position was contested notably by U.S. Solicitor General James Lee Rankin (in office 1956–1961), but in Jacobellis v. Ohio Stewart concluded that criminal obscenity laws are constitutionally limited under the First and Fourteenth Amendments to hardcore pornography.
Concurring in the 1957 Roth v. United States Justice John Marshall Harlan II wrote that "even assuming that pornography cannot be deemed ever to cause, in an immediate sense, criminal sexual conduct, other interests within the proper cognizance of the States may be protected by the prohibition placed on such materials."
The 1967 Public Law 90-100 found the traffic in pornography to be "a matter of national concern", as well as in obscenity. In this period the Court considered pornography to have two major dimensions:
- The first can be defined as dealing with sexual representations that are offensive to public morality or taste, which concerned the Court notably in the 1966 Ginzburg v. United States case.
- The second centers on the effect of pornography on specific individuals or classes, which is the focus of most public discussions and prior Court pornography decisions. This dimension was mentioned only twice in the array of decisions made in 1966.
A frustration was expressed notably by Justice Hugo Black in the 1966 Mishkin v. New York: "I wish once more to express my objections to saddling this Court with the irksome and inevitably unpopular and unwholesome task of finally deciding by a case-by-case, sight-by-sight personal judgment of the members of this Court what pornography (whatever that means) is too hard core for people to see or read."
In the 1974 Hamling v. United States decision the Supreme Court said that just because pornographic materials are for sale and purchased around the country, "Mere availability of similar materials by itself means nothing more than that other persons are engaged in similar activities."
The 1976 American Heritage Dictionary of the English Language defined that pornography consists of "written, graphic, or other forms of communication intended to excite lascivious feelings". Since determining what is pornography and what is "soft core" and "hard core" are subjective questions to judges, juries, and law enforcement officials, it is difficult to define, since the law cases cannot print examples for the courts to follow.
The Rehnquist Court further enhanced the power of community controls on pornography. Current Chief Justice John Roberts told at the confirmation hearing on his nomination: "Well, Senator, it's my understanding under the Supreme Court's doctrine that pornographic expression is not protected to the same extent at least as political and core speech, and the difficulty that the Court has addressed in these different areas of course is always defining what is or is not pornography and what is entitled to protection under the First Amendment and what is not".
The famous Indianapolis definition of pornography by Dworkin and MacKinnon paralleled their Minneapolis ordinance. The first was rejected by the United States Court of Appeals for the Seventh Circuit for several reasons. The ordinance did not use any of the accepted terms that the Supreme Court had developed over time for determining when material is obscene, including "prurient interest", "offensiveness", or "local community standards".
Another concern was the way the women were depicted in the work. If women were referred to in the approved fashion stressing equality, the activity involved would be regardless of how sexually explicit it was.The Court also indicated that if women were referred to in a disapproving way depicting them as subversive or as enjoying humiliation, the activity would be unlawful regardless of the "literary, artistic or political qualities of the work taken as a whole".
Judge Frank Easterbrook said: "We accept the premises of this legislation. Depictions of subordination tend to perpetuate subordination. The subordinate status of women in turn leads to affront and lower pay at work, insult and injury at home, battery and rape on the streets.... Yet this simply demonstrates the power of pornography as speech."
Conceptions of Democracy in American Constitutional Argument: The Case of Pornography Regulation by Frank Michelman, issued by Tennessee Law Review (vol. 56, no. 291, 1989) partially consented that "pornography is political expression in that it promulgates a certain view of women's natures and thus of women's appropriate relations and treatment in society", but also concluded that the Indianapolis ordinance was precisely designed to suppress that particular view by censoring pornography.
Minneapolis ordinance was struck down on the grounds that it was ambiguous and vague, however, despite of its failure the proposal influenced other communities across the United States.
In May 2005 U.S. Attorney General Alberto Gonzales established an Obscenity Prosecution Task Force. The task force, according to a Department of Justice news release on May 5, was "dedicated to the investigation and prosecution of the distributors of hard-core pornography that meets the test for obscenity, as defined by the United States Supreme Court."
Under President Bush's and Gonzales' rationales the FBI Adult Obscenity Squad was recruited in August 2005 to gather evidence against "manufacturers and purveyors" of adult pornography.
Child pornography:
Main articles:
- Child pornography laws in the United States
- Legal status of cartoon pornography depicting minors § United States
The 1970 Lockhart Commission recommended eliminating all criminal penalties for pornography except for pornographic depictions of minors, or sale of pornography to minors.
However, prior to 1977, only two states had laws which prohibited the use of children in the production or distribution of pornographic materials or performances.
In 1977, the Department of Justice strongly endorsed legislation which banned the production and dissemination of child pornography. These efforts have been unsuccessfully challenged in the 1982 New York v. Ferber case ("The States are entitled to greater leeway in the regulation of pornographic depictions of children...").
Although the states have a different age of consent, in accordance with the Federal Labeling and Record-Keeping Law all models featured in pornographic content should be at least 18 years of age. This kind of material is often labeled as "adult" and the appropriate disclaimers are common.
They are based on what "depicts or describes, in terms patently offensive as measured by contemporary community standards, sexual or excretory activities or organs".
It is a federal crime to possess, distribute, or produce non-fictional child pornography and carries large fines and prison sentences of up to 30 years upon conviction and requirement to register as a sex offender.
Anti-pornography movement:
Main article: Anti-pornography movement in the United States
An anti-pornography movement has existed in the United States since before the 1969 Supreme Court decision of Stanley v. Georgia, which held that people could view whatever they wished in the privacy of their own homes, by establishing an implied "right to privacy" in U.S. law. This led President Lyndon B. Johnson, with the backing of Congress, to appoint a commission to study pornography.
The anti-pornography movement seeks to maintain or restore restrictions and to increase or create restrictions on the production, sale or dissemination of pornography.
Jesuit priest Father Morton A. Hill (1917-1985) was a leader of the campaign against pornography in the United States in the 1960s, 1970s and 1980s. He was one of the founders of Morality in Media, which was created in 1962 to fight pornography.
Morality in Media was launched by an interfaith group of clergy and Hill was president until his death in 1985. Morality in Media continues with Patrick A. Trueman, a registered federal lobbyist, as president.
So prominent was Hill on the issue, that in 1969 President Lyndon B. Johnson appointed him to the President's Commission on Obscenity and Pornography. Father Hill and another clergyman on the commission, Dr. Winfrey C. Link, believed that the commission was stacked with supporters of loosening laws on pornography, and issued the Hill-Link Minority Report rebutting the conclusions of the majority report, which held that pornography should be decriminalized as there were no links between it and criminal behavior.
The majority report was widely criticized and rejected by Congress. The Senate rejected the commission's findings and recommendations by a 60–5 vote, with 34 abstentions. President Nixon, who had succeeded Johnson in 1969, also emphatically rejected the majority report.
The Hill-Link Minority Report, on the other hand, which recommended maintaining anti-obscenity statutes, was read into the record of both the United States Senate and the United States House of Representatives. It was cited by the Burger Court in its 1973 obscenity decisions, including Miller v. California.
See also:
- Pornography: Encyclopedia of Everyday Law
- Attorney General's Commission on Pornography Final Report, July 1986, U.S. Department of Justice, Washington D.C.
- Might Pornography Cause Harm? by Anne W. Eaton, The University of Chicago
- White House Protection From Pornography Week, 2003
- American Porn. Report by Frontline (PBS TV series) (first aired in 2002, updated in 2004), watchable online.
- Deep Inside : A study of 10,000 Porn Stars and Their Careers (2013)
Sexual Attraction
- YouTube Video: This Is What Sexual Attraction Looks Like
- YouTube Video: Sexual Arousal, Desire and Attraction: What's the Difference?
- YouTube Video: Sex & Relationships : Understanding the Science of Sexual Attraction
* -- What Determines Sexual Attraction?
By Brittany Loggins @ verywellmind
Updated on January 26, 2022
Medically reviewed by Ivy Kwong, LMFT
First up, let's talk about what sexual attraction is. According to the LBGT Center at the University of North Carolina Chapel Hill, sexual attraction is "attraction that makes people desire sexual contact or shows sexual interest in another person(s)."
Pretty self-explanatory, right? What's less self-explanatory is how it happens. Everyone has been in the situation of not understanding why they are or aren't attracted to another person, and it turns out science has a lot to do with why.
This article explores the many factors that affect your level of attraction to other people.
What Is Physical Attraction?
Biological Factors That Affect Attraction:
When you meet someone new, it might be difficult to discern why you find yourself attracted to (or not attracted to) them. However, studies show that biology has a lot to do with your level of attraction to someone else.
Adrenaline and Excitement:
Let's talk about one of the cornerstone studies in the psychology field regarding attraction: The Love Bridge study. This study made the connection between arousal and attraction. In this study, psychologists Donald Dutton and Arthur Aron had 85 men walk across either a scary suspension bridge or a sturdy regular bridge.
On the bridge, the men were approached by a female interviewer who asked them to fill out questionnaires in response to pictures. After each interview, she passed along her phone number. It turns out, people who were on the scary bridge were much more likely to call and put down sexual content and imagery on their responses to the questionnaire. This is an example of the misattribution of arousal.
In other words, they were excited about something, and that person was there for them to project their excitement on. Looking back, it's likely that the men just remembered feeling excited and then seeing a pretty woman.
Another study showed a photo of a moderately attractive person to people getting on or off of a roller coaster. They asked the people to rate the photo in terms of attractiveness and dating desirability. They were also asked to rate their seatmate's desirability. The people getting off the roller coaster rated their seatmates higher in terms of attractiveness than those getting on the roller coaster.
What Is Sexual Tension?
Natural Scent:
In addition to adrenaline, studies have found that smell plays a role in attraction. For example, after being asked to smell different t-shirts worn by men, women actually chose the shirts of men whose genes signified their immune systems were different from their own.
Then, of course, there's always the case for pheromones, which is a natural scent that your body produces.
Psychological Factors That Affect Attraction:
Aside from biology, psychology plays a role in how attractive you perceive someone else to be.
Mood:
Justin Lehmiller, PhD, a social psychologist, notes that people tend to be drawn to partners who are psychologically similar to themselves. He expands on this by saying that mood can impact the level of attraction you feel toward someone.
For example, if you've just received great news, you're more likely to like the next person you meet more than you normally would. This, Lehmiller says, can impact whether or not you're likely to develop an attraction to them.
Attachment Style, Values, and Emotions:
Patrick Wanis, PhD, human behavior and relationship expert, says that attachment styles can also greatly impact attraction. On his blog, he suggests that “we subconsciously become attracted to people who will reflect and reinforce our beliefs and expectations about caring, trust, abandonment, dependence, support, intimacy, vulnerability.”
Wanis also believes that people search for partners with similar values and beliefs and people at similar life stages.
Another study supported the idea that people look for similarities in terms of attraction. It found that people were more drawn to others whose emotions and motivations felt familiar.
The study had people watch others as they experienced different emotions. It found that they were more likely to be attracted to people whose emotions they could understand without it being explicitly stated.
Winning Someone Over:
Finally, while everyone can agree that it's nice to be liked, one study found that people also like the idea of winning someone over. The study asked co-ed students to eavesdrop on their partner and another group.
While they liked it when they found out that their partner had a positive impression of them, they actually liked it even more when they found out that the person's impression of them had started negatively and turned positive. This way, the person felt like their partner's feelings were more indicative of their true feelings about their personality.
My Partner Doesn’t Find Me Attractive Anymore:
Other Factors:
While you can't control biological and psychological factors, there are some things you have a bit more control over in terms of how attractive you find other people. Here are a few of those factors.
Location:
Where you live can impact your level of attraction to others in terms of proximity to people and access to different types of people. This can be as simple as who is available at the moment (think of your neighbor from the college dorm).
One study showed that women from healthier countries preferred men with more feminine qualities, whereas women from developing nations preferred men with more traditionally masculine features. The study actually found that across 30 countries, as the country's health decreased, the preferences for masculinity increased.
Scarcity:
Lehmiller also references the idea of scarcity and uses the example of the "closing time effect," which suggests that people at a bar will rate other patrons as more attractive the closer they get to closing time. Basically, the more limited the options become, the more likely people are to settle for whatever is available at the time.
Familial Relationships:
Of course, physical preferences can be shaped by past experiences with similar-looking people, as well as a person's relationship with their family. In other words, if you grew up in a home with a father who was more traditionally masculine, that may be what you consider attractive if you have a good relationship with your father. To you, masculinity may also denote kindness and acceptance.
A Word From Verywell:
While there have been lots of studies on what people find attractive, a big part of it is still dependent on your personal preferences and past experiences. If you are currently looking for a partner, I hope this encourages you as opposed to discouraging you. Think of it this way: biology takes care of a lot of the heavy lifting for you, if you are willing to pay attention to it.
By Brittany Loggins
Brittany is a health and lifestyle writer and former staffer at TODAY on NBC and CBS News. She's also contributed to dozens of magazines.
___________________________________________________________________________
Sexual attraction (Wikipedia)
Sexual attraction is attraction on the basis of sexual desire or the quality of arousing such interest. Sexual attractiveness or sex appeal is an individual's ability to attract other people sexually, and is a factor in sexual selection or mate choice.
The attraction can be to the physical or other qualities or traits of a person, or to such qualities in the context where they appear. The attraction may be to a person's aesthetics, movements, voice, or smell, among other things. The attraction may be enhanced by a person's adornments, clothing, perfume or style.
It can be influenced by individual genetic, psychological, or cultural factors, or to other, more amorphous qualities. Sexual attraction is also a response to another person that depends on a combination of the person possessing the traits and on the criteria of the person who is attracted.
Though attempts have been made to devise objective criteria of sexual attractiveness and measure it as one of several bodily forms of capital asset (see erotic capital), a person's sexual attractiveness is to a large extent a subjective measure dependent on another person's interest, perception, and sexual orientation.
For example, a gay or lesbian person would typically find a person of the same sex to be more attractive than one of the other sex. A bisexual person would find either sex to be attractive. Asexuality refers to those who do not experience sexual attraction for either sex, though they may have romantic attraction or a non-directed libido.
Interpersonal attraction includes factors such as physical or psychological similarity, familiarity or possessing a preponderance of common or familiar features, similarity, complementarity, reciprocal liking, and reinforcement.
The ability of a person's physical and other qualities to create a sexual interest in others is the basis of their use in advertising, film, and other visual media, as well as in modeling and other occupations.
In evolutionary terms, the ovulatory shift hypothesis posits that female humans exhibit different sexual behaviours and desires at points in their menstrual cycle, as a means to ensure that they attract a high quality mate to copulate with during their most fertile time.
Hormone levels throughout the menstrual cycle affect a woman's overt behaviours, influencing the way a woman presents herself to others during stages of her menstrual cycle, in an attempt to attract high quality mates the closer the woman is to ovulation.
Social and biological factors:
Human sexuality has many aspects. In biology, sexuality describes the reproductive mechanism and the basic biological drive that exists in all sexually reproducing species and can encompass sexual intercourse and sexual contact in all its forms.
There are also emotional and physical aspects of sexuality. These relate to the bond between individuals, which may be expressed through profound feelings or emotions. Sociologically, it can cover the cultural, political, and legal aspects; philosophically, it can span the moral, ethical, theological, spiritual, and religious aspects.
Which aspects of a person's sexuality attract another is influenced by cultural factors; it has varied over time, as well as personal factors. Influencing factors may be determined more locally among sub-cultures, across sexual fields, or simply by the preferences of the individual. These preferences come about as a result of a complex variety of genetic, psychological, and cultural factors.
A person's physical appearance has a critical impact on their sexual attractiveness. This involves the impact one's appearance has on the senses, especially in the beginning of a relationship, among them:
As with other animals, pheromones may have an impact, though less significantly in the case of humans. Theoretically, the "wrong" pheromone may cause someone to be disliked, even when they would otherwise appear attractive. Frequently, a pleasant-smelling perfume is used to encourage the other person to more deeply inhale the air surrounding its wearer, increasing the probability that the individual's pheromones will be inhaled.
The importance of pheromones in human relationships is probably limited and is widely disputed, although it appears to have some scientific basis.
Some people exhibit high levels of sexual fetishism and are sexually stimulated by other stimuli not normally associated with sexual arousal. The degree to which such fetishism exists or has existed in different cultures is controversial.
Pheromones have been determined to play a role in sexual attraction between people. They influence gonadal hormone secretion, for example, follicle maturation in the ovaries in females and testosterone and sperm production in males.
High anxiety:
Research conducted by Donald G. Dutton and Arthur P. Aron in the 1970s aimed to find the relation between sexual attraction and high anxiety conditions. In doing so, 85 male participants were contacted by an attractive female interviewer at either a fear-arousing suspension bridge or a normal bridge.
Conclusively, it was shown that the male participants who were asked by the female interviewer to perform the thematic apperception test (TAT) on the fear-arousing bridge, wrote more sexual content in the stories and attempted, with greater effort, to contact the interviewer after the experiment than those participants who performed the TAT on the normal bridge.
In another test, a male participant, chosen from a group of 80, was given anticipated shocks. With him was an attractive female confederate, who was also being shocked. The experiment showed that the male's sexual imagery in the TAT was much higher when self shock was anticipated and not when the female confederate shock was anticipated.
Enhancement:
People consciously or subconsciously enhance their sexual attractiveness or sex appeal for a number of reasons. It may be to attract someone with whom they can form a deeper relationship, for companionship, procreation, or an intimate relationship, besides other possible purposes.
It can be part of a courtship process. This can involve physical aspects or interactive processes whereby people find and attract potential partners, and maintain a relationship.
These processes, which involve attracting a partner and maintaining sexual interest, can include flirting, which can be used to attract the sexual attention of another to encourage romance or sexual relations, and can involve body language, conversation, joking, or brief physical contact.
Sex and sexuality differences:
Men have been found to have a greater interest in uncommitted sex compared to women. Some research shows this interest to be more sociological than biological. Men have a greater interest in visual sexual stimuli than women.
However, additional trends have been found with a greater sensitivity to partner status in women choosing a sexual partner and men placing a greater emphasis on physical attractiveness in a potential mate, as well as a significantly greater tendency toward sexual jealousy in men and emotional jealousy in women.
Bailey, Gaulin, Agyei, and Gladue (1994) analyzed whether these results varied according to sexual orientation. In general, they found biological sex played a bigger role in the psychology of sexual attraction than orientation. However, there were some differences between homosexual and heterosexual women and men on these factors.
While gay and straight men showed similar psychological interest in casual sex on markers of sociosexuality, gay men showed a larger number of partners in behaviour expressing this interest (proposed to be due to a difference in opportunity). Self-identified lesbian women showed a significantly greater interest in visual sexual stimuli than heterosexual women and judged partner status to be less important in romantic partnerships.
Heterosexual men had a significantly greater preference for younger partners than homosexual men. People who identify as asexual may not be sexually attracted to anyone. Gray asexuality includes those who only experience sexual attraction under certain circumstances; for example, exclusively after an emotional bond has been formed.
This tends to vary from person to person.
Sexual preferences and hormonesThe ovulatory shift hypothesis is the theory that female humans tend to exhibit different sexual behaviours and desires at points in their cycle.
Two meta-analyses published in 2014 reached opposing conclusions on whether the existing evidence was robust enough to support the prediction that women's mate preferences change across the cycle. A newer 2018 review does not show women changing the type of men they desire at different times in their fertility cycle.
In males, a masculine face has been positively correlated with fewer respiratory diseases and, as a consequence, masculine features offer a marker of health and reproductive success.
Ovulation and ornamentation:
Hormone levels throughout the menstrual cycle affect a woman's behaviour in preferences and in their overt behaviours. The ornamentation effect is a phenomenon influenced by a stage of the menstrual cycle which refers to the way a woman presents herself to others, in a way to attract potential sexual partners.
Studies have found that the closer women were to ovulation, the more provocatively they dress and the more attractive they are rated.
It is possible that women are sensitive to the changes in their physical attractiveness throughout their cycles, such that at their most fertile stages their levels of attractiveness are increased. Consequently, they choose to display their increased levels of attractiveness through this method of ornamentation.
During periods of hormonal imbalance, women exhibit a peak in sexual activity. As these findings have been recorded for female-initiated sexual activity and not for male-initiated activity, the causation appears to be hormonal changes during the menstrual cycle.
Research has also found that menstrual cycles affect sexual behaviour frequency in pre-menopausal women. For example, women who had weekly sexual intercourse with men had menstrual cycles with the average duration of 29 days, while women with less frequent sexual interactions tended to have more extreme cycle lengths.
Male response to ovulation:
Changes in hormones during a female's cycles affect the way she behaves and the way males behave towards her. Research has found that men are a lot more attentive and loving towards their partners when they are in the most fertile phase of their cycles, in comparison to when they are in the luteal phases.
Men become increasingly jealous and possessive over their partners during this stage.
See also:
By Brittany Loggins @ verywellmind
Updated on January 26, 2022
Medically reviewed by Ivy Kwong, LMFT
First up, let's talk about what sexual attraction is. According to the LBGT Center at the University of North Carolina Chapel Hill, sexual attraction is "attraction that makes people desire sexual contact or shows sexual interest in another person(s)."
Pretty self-explanatory, right? What's less self-explanatory is how it happens. Everyone has been in the situation of not understanding why they are or aren't attracted to another person, and it turns out science has a lot to do with why.
This article explores the many factors that affect your level of attraction to other people.
What Is Physical Attraction?
Biological Factors That Affect Attraction:
When you meet someone new, it might be difficult to discern why you find yourself attracted to (or not attracted to) them. However, studies show that biology has a lot to do with your level of attraction to someone else.
Adrenaline and Excitement:
Let's talk about one of the cornerstone studies in the psychology field regarding attraction: The Love Bridge study. This study made the connection between arousal and attraction. In this study, psychologists Donald Dutton and Arthur Aron had 85 men walk across either a scary suspension bridge or a sturdy regular bridge.
On the bridge, the men were approached by a female interviewer who asked them to fill out questionnaires in response to pictures. After each interview, she passed along her phone number. It turns out, people who were on the scary bridge were much more likely to call and put down sexual content and imagery on their responses to the questionnaire. This is an example of the misattribution of arousal.
In other words, they were excited about something, and that person was there for them to project their excitement on. Looking back, it's likely that the men just remembered feeling excited and then seeing a pretty woman.
Another study showed a photo of a moderately attractive person to people getting on or off of a roller coaster. They asked the people to rate the photo in terms of attractiveness and dating desirability. They were also asked to rate their seatmate's desirability. The people getting off the roller coaster rated their seatmates higher in terms of attractiveness than those getting on the roller coaster.
What Is Sexual Tension?
Natural Scent:
In addition to adrenaline, studies have found that smell plays a role in attraction. For example, after being asked to smell different t-shirts worn by men, women actually chose the shirts of men whose genes signified their immune systems were different from their own.
Then, of course, there's always the case for pheromones, which is a natural scent that your body produces.
Psychological Factors That Affect Attraction:
Aside from biology, psychology plays a role in how attractive you perceive someone else to be.
Mood:
Justin Lehmiller, PhD, a social psychologist, notes that people tend to be drawn to partners who are psychologically similar to themselves. He expands on this by saying that mood can impact the level of attraction you feel toward someone.
For example, if you've just received great news, you're more likely to like the next person you meet more than you normally would. This, Lehmiller says, can impact whether or not you're likely to develop an attraction to them.
Attachment Style, Values, and Emotions:
Patrick Wanis, PhD, human behavior and relationship expert, says that attachment styles can also greatly impact attraction. On his blog, he suggests that “we subconsciously become attracted to people who will reflect and reinforce our beliefs and expectations about caring, trust, abandonment, dependence, support, intimacy, vulnerability.”
Wanis also believes that people search for partners with similar values and beliefs and people at similar life stages.
Another study supported the idea that people look for similarities in terms of attraction. It found that people were more drawn to others whose emotions and motivations felt familiar.
The study had people watch others as they experienced different emotions. It found that they were more likely to be attracted to people whose emotions they could understand without it being explicitly stated.
Winning Someone Over:
Finally, while everyone can agree that it's nice to be liked, one study found that people also like the idea of winning someone over. The study asked co-ed students to eavesdrop on their partner and another group.
While they liked it when they found out that their partner had a positive impression of them, they actually liked it even more when they found out that the person's impression of them had started negatively and turned positive. This way, the person felt like their partner's feelings were more indicative of their true feelings about their personality.
My Partner Doesn’t Find Me Attractive Anymore:
Other Factors:
While you can't control biological and psychological factors, there are some things you have a bit more control over in terms of how attractive you find other people. Here are a few of those factors.
Location:
Where you live can impact your level of attraction to others in terms of proximity to people and access to different types of people. This can be as simple as who is available at the moment (think of your neighbor from the college dorm).
One study showed that women from healthier countries preferred men with more feminine qualities, whereas women from developing nations preferred men with more traditionally masculine features. The study actually found that across 30 countries, as the country's health decreased, the preferences for masculinity increased.
Scarcity:
Lehmiller also references the idea of scarcity and uses the example of the "closing time effect," which suggests that people at a bar will rate other patrons as more attractive the closer they get to closing time. Basically, the more limited the options become, the more likely people are to settle for whatever is available at the time.
Familial Relationships:
Of course, physical preferences can be shaped by past experiences with similar-looking people, as well as a person's relationship with their family. In other words, if you grew up in a home with a father who was more traditionally masculine, that may be what you consider attractive if you have a good relationship with your father. To you, masculinity may also denote kindness and acceptance.
A Word From Verywell:
While there have been lots of studies on what people find attractive, a big part of it is still dependent on your personal preferences and past experiences. If you are currently looking for a partner, I hope this encourages you as opposed to discouraging you. Think of it this way: biology takes care of a lot of the heavy lifting for you, if you are willing to pay attention to it.
By Brittany Loggins
Brittany is a health and lifestyle writer and former staffer at TODAY on NBC and CBS News. She's also contributed to dozens of magazines.
___________________________________________________________________________
Sexual attraction (Wikipedia)
Sexual attraction is attraction on the basis of sexual desire or the quality of arousing such interest. Sexual attractiveness or sex appeal is an individual's ability to attract other people sexually, and is a factor in sexual selection or mate choice.
The attraction can be to the physical or other qualities or traits of a person, or to such qualities in the context where they appear. The attraction may be to a person's aesthetics, movements, voice, or smell, among other things. The attraction may be enhanced by a person's adornments, clothing, perfume or style.
It can be influenced by individual genetic, psychological, or cultural factors, or to other, more amorphous qualities. Sexual attraction is also a response to another person that depends on a combination of the person possessing the traits and on the criteria of the person who is attracted.
Though attempts have been made to devise objective criteria of sexual attractiveness and measure it as one of several bodily forms of capital asset (see erotic capital), a person's sexual attractiveness is to a large extent a subjective measure dependent on another person's interest, perception, and sexual orientation.
For example, a gay or lesbian person would typically find a person of the same sex to be more attractive than one of the other sex. A bisexual person would find either sex to be attractive. Asexuality refers to those who do not experience sexual attraction for either sex, though they may have romantic attraction or a non-directed libido.
Interpersonal attraction includes factors such as physical or psychological similarity, familiarity or possessing a preponderance of common or familiar features, similarity, complementarity, reciprocal liking, and reinforcement.
The ability of a person's physical and other qualities to create a sexual interest in others is the basis of their use in advertising, film, and other visual media, as well as in modeling and other occupations.
In evolutionary terms, the ovulatory shift hypothesis posits that female humans exhibit different sexual behaviours and desires at points in their menstrual cycle, as a means to ensure that they attract a high quality mate to copulate with during their most fertile time.
Hormone levels throughout the menstrual cycle affect a woman's overt behaviours, influencing the way a woman presents herself to others during stages of her menstrual cycle, in an attempt to attract high quality mates the closer the woman is to ovulation.
Social and biological factors:
Human sexuality has many aspects. In biology, sexuality describes the reproductive mechanism and the basic biological drive that exists in all sexually reproducing species and can encompass sexual intercourse and sexual contact in all its forms.
There are also emotional and physical aspects of sexuality. These relate to the bond between individuals, which may be expressed through profound feelings or emotions. Sociologically, it can cover the cultural, political, and legal aspects; philosophically, it can span the moral, ethical, theological, spiritual, and religious aspects.
Which aspects of a person's sexuality attract another is influenced by cultural factors; it has varied over time, as well as personal factors. Influencing factors may be determined more locally among sub-cultures, across sexual fields, or simply by the preferences of the individual. These preferences come about as a result of a complex variety of genetic, psychological, and cultural factors.
A person's physical appearance has a critical impact on their sexual attractiveness. This involves the impact one's appearance has on the senses, especially in the beginning of a relationship, among them:
- Visual perception (the symmetry of the face, physical attractiveness, health, and how they act or move, for example, while dancing);
- Audition (how the other's voice and movements sound);
- Olfaction (how the other smells, naturally or artificially; the wrong smell may be repellent);
- Somatosensory system (for example touch and temperature).
As with other animals, pheromones may have an impact, though less significantly in the case of humans. Theoretically, the "wrong" pheromone may cause someone to be disliked, even when they would otherwise appear attractive. Frequently, a pleasant-smelling perfume is used to encourage the other person to more deeply inhale the air surrounding its wearer, increasing the probability that the individual's pheromones will be inhaled.
The importance of pheromones in human relationships is probably limited and is widely disputed, although it appears to have some scientific basis.
Some people exhibit high levels of sexual fetishism and are sexually stimulated by other stimuli not normally associated with sexual arousal. The degree to which such fetishism exists or has existed in different cultures is controversial.
Pheromones have been determined to play a role in sexual attraction between people. They influence gonadal hormone secretion, for example, follicle maturation in the ovaries in females and testosterone and sperm production in males.
High anxiety:
Research conducted by Donald G. Dutton and Arthur P. Aron in the 1970s aimed to find the relation between sexual attraction and high anxiety conditions. In doing so, 85 male participants were contacted by an attractive female interviewer at either a fear-arousing suspension bridge or a normal bridge.
Conclusively, it was shown that the male participants who were asked by the female interviewer to perform the thematic apperception test (TAT) on the fear-arousing bridge, wrote more sexual content in the stories and attempted, with greater effort, to contact the interviewer after the experiment than those participants who performed the TAT on the normal bridge.
In another test, a male participant, chosen from a group of 80, was given anticipated shocks. With him was an attractive female confederate, who was also being shocked. The experiment showed that the male's sexual imagery in the TAT was much higher when self shock was anticipated and not when the female confederate shock was anticipated.
Enhancement:
People consciously or subconsciously enhance their sexual attractiveness or sex appeal for a number of reasons. It may be to attract someone with whom they can form a deeper relationship, for companionship, procreation, or an intimate relationship, besides other possible purposes.
It can be part of a courtship process. This can involve physical aspects or interactive processes whereby people find and attract potential partners, and maintain a relationship.
These processes, which involve attracting a partner and maintaining sexual interest, can include flirting, which can be used to attract the sexual attention of another to encourage romance or sexual relations, and can involve body language, conversation, joking, or brief physical contact.
Sex and sexuality differences:
Men have been found to have a greater interest in uncommitted sex compared to women. Some research shows this interest to be more sociological than biological. Men have a greater interest in visual sexual stimuli than women.
However, additional trends have been found with a greater sensitivity to partner status in women choosing a sexual partner and men placing a greater emphasis on physical attractiveness in a potential mate, as well as a significantly greater tendency toward sexual jealousy in men and emotional jealousy in women.
Bailey, Gaulin, Agyei, and Gladue (1994) analyzed whether these results varied according to sexual orientation. In general, they found biological sex played a bigger role in the psychology of sexual attraction than orientation. However, there were some differences between homosexual and heterosexual women and men on these factors.
While gay and straight men showed similar psychological interest in casual sex on markers of sociosexuality, gay men showed a larger number of partners in behaviour expressing this interest (proposed to be due to a difference in opportunity). Self-identified lesbian women showed a significantly greater interest in visual sexual stimuli than heterosexual women and judged partner status to be less important in romantic partnerships.
Heterosexual men had a significantly greater preference for younger partners than homosexual men. People who identify as asexual may not be sexually attracted to anyone. Gray asexuality includes those who only experience sexual attraction under certain circumstances; for example, exclusively after an emotional bond has been formed.
This tends to vary from person to person.
Sexual preferences and hormonesThe ovulatory shift hypothesis is the theory that female humans tend to exhibit different sexual behaviours and desires at points in their cycle.
Two meta-analyses published in 2014 reached opposing conclusions on whether the existing evidence was robust enough to support the prediction that women's mate preferences change across the cycle. A newer 2018 review does not show women changing the type of men they desire at different times in their fertility cycle.
In males, a masculine face has been positively correlated with fewer respiratory diseases and, as a consequence, masculine features offer a marker of health and reproductive success.
Ovulation and ornamentation:
Hormone levels throughout the menstrual cycle affect a woman's behaviour in preferences and in their overt behaviours. The ornamentation effect is a phenomenon influenced by a stage of the menstrual cycle which refers to the way a woman presents herself to others, in a way to attract potential sexual partners.
Studies have found that the closer women were to ovulation, the more provocatively they dress and the more attractive they are rated.
It is possible that women are sensitive to the changes in their physical attractiveness throughout their cycles, such that at their most fertile stages their levels of attractiveness are increased. Consequently, they choose to display their increased levels of attractiveness through this method of ornamentation.
During periods of hormonal imbalance, women exhibit a peak in sexual activity. As these findings have been recorded for female-initiated sexual activity and not for male-initiated activity, the causation appears to be hormonal changes during the menstrual cycle.
Research has also found that menstrual cycles affect sexual behaviour frequency in pre-menopausal women. For example, women who had weekly sexual intercourse with men had menstrual cycles with the average duration of 29 days, while women with less frequent sexual interactions tended to have more extreme cycle lengths.
Male response to ovulation:
Changes in hormones during a female's cycles affect the way she behaves and the way males behave towards her. Research has found that men are a lot more attentive and loving towards their partners when they are in the most fertile phase of their cycles, in comparison to when they are in the luteal phases.
Men become increasingly jealous and possessive over their partners during this stage.
See also:
Erogenous Zone
- YouTube Video: Friends (TV Sitcom) - The Erogenous Zones Of Women
- YouTube Video: Monica's 7 Erogenous Zones | Friends (TV Sitcom)
- YouTube Video: The Steam Room Incident | Friends (TV Sitcom)
An erogenous zone (from Greek ἔρως, érōs "love"; and English -genous "producing", from Greek -γενής, -genḗs "born") is an area of the human body that has heightened sensitivity, the stimulation of which may generate a sexual response, such as relaxation, sexual fantasies, sexual arousal and orgasm.
Erogenous zones are located all over the human body, but the sensitivity of each varies, and depends on concentrations of nerve endings that can provide pleasurable sensations when stimulated. The touching of another person's erogenous zone is regarded as an act of physical intimacy.
Whether a person finds stimulation in these areas to be pleasurable or objectionable depends on a range of factors, including their level of arousal, the circumstances in which it takes place, the cultural context, the nature of the relationship between the partners, and the partners' personal histories.
Erogenous zones may be classified by the type of sexual response that they generate. Many people are gently aroused when their eyelids, eyebrows, temples, shoulders, hands, arms, and hair are subtly touched.
Gently touching or stroking of these zones stimulates a partner during foreplay and increases the arousal level. Also, the gentle massage or stroke of the abdominal area along with kissing or simply touching the navel can be a type of stimulation.
Classification:
Specific zones:
Specific zones are associated with sexual response, and include the lips and nipples in addition to areas of the genitals, notably corona of the glans penis, clitoris and rest of the vulva, and perianal skin.
These zones have a high density of innervation, and may have an efficiency of wound healing and a capacity to stimulate generalized cerebral arousal.
Nonspecific zones:
In these zones, the skin is similar to normal-haired skin and has the normal high density of nerves and hair follicles. These areas include the sides and back of the neck, the inner arms, the axillae (armpits) and sides of the thorax (chest).
Genitals:
Male:
Males can be aroused by stimulation to the sides of the glans and penis, upper side of the glans, the front side of the scrotum, the skin between the scrotum and anus perineum, and around the anus.
Female:
Parts of the vulva, especially the clitoris, are erogenous zones. While the vagina is not especially sensitive as a whole, its lower third (the area close to the entrance) has concentrations of the nerve endings that can provide pleasurable sensations during sexual activity when stimulated; this is also called the anterior wall of the vagina or the outer one-third of the vagina, and it contains the majority of the vaginal nerve endings, making it more sensitive to touch than the inner two-thirds of the vaginal barrel.
Within the anterior wall of the vagina, there is a patch of ribbed rough tissue which has a texture that is sometimes described as similar to the palate (the roof of a mouth) or a raspberry, and may feel spongy when a woman is sexually aroused.
This is the urethral sponge, which may also be the location of an area that some women report is an erogenous zone; this is sometimes called the G-spot. When stimulated, it may lead to sexual arousal, an orgasm, or female ejaculation.
The existence of the G-spot and whether or not it is a distinct structure is debated among researchers, as reports of its location vary from woman to woman, it appears to be nonexistent in some women, and scientists commonly believe that it is an extension of the clitoris.
Head:
Mouth:
The lips and tongue are sensitive and can be stimulated by kissing and licking. Biting at the lip can also provide stimulus.
Neck:
The neck, clavicle area and the back of the neck are very sensitive, and can be stimulated by licking, kissing or light caressing. Some people also like being bitten gently in these areas, often to the point that a "hickey", or "love-bite" is formed.
Ears:
Some people find whispering or breathing softly in the ear to be pleasurable and relaxing, as well as licking, biting, caressing and/or kissing it especially the area of and behind the earlobe.
Torso:
Chest:
The areola and nipple contain Golgi-Mazzoni, Vater-Pacini and genital corpuscles. No Meissner's corpuscles and few organized nerve endings are present. There are concentrations of nerve tissue in the area of ducts and masses of smooth muscle.
The hair surrounding the areola adds additional sensory tissue. The mass of smooth muscle and glandular-duct tissue in the nipple and areola block the development of normal dermal nerve networks which are present in other erogenous regions and the development of special end organs.
The entire breast has a network of nerve endings, and it has the same number of nerve endings no matter how large the breast is, so that larger breasts may need more stimulation than smaller ones.
Intense nipple stimulation may result in a surge in the production of oxytocin and prolactin which could have a significant effect on the individual's genitals, even to the point that some people of both sexes can achieve orgasm through nipple stimulation alone.
Having the chest, breasts and nipples stimulated manually (hands), digitally (fingers, toes) and/or orally (mouth, lips, teeth, tongue) is a pleasurable experience for many people of both sexes.
Abdomen and navel:
Main articles: Navel fetishism and Alvinolagnia.
Many people find stimulation (kissing, biting, scratching, tickling, caressing) of the abdomen to be pleasurable, especially close to the pubic region. It can cause strong arousal in men and women, in some even stronger than stimulation of the genitals. The navel is one of the many erogenous zones that has heightened sensitivity.
In a 1982 study of eroticism in dress entitled "Skin to Skin", Prudence Glynn claimed that the waist symbolized virginity and that it was the first place that a man would touch a woman "when indicating more than a formal courtesy".
The navel and the region below when touched by the finger or the tip of the tongue result in the production of erotic sensations.
Arms:
The skin of the arms, and specifically the softer skin of the inner arms and across the creased mid-arm bend covering the ventral side of the elbow, are highly sensitive to manual or oral stimulation.
Caressing with fingers or tongue, more vigorous kneading, and butterfly kissing can initiate arousal and, in some cases, induce clitoral/vaginal orgasm or penile ejaculation without direct contact with the latter areas.
The mid-arm bend is especially sensitive due to the thinner skin found there, which makes nerve endings more accessible. Arm sensitivity may be reduced or concentrated to a more narrow range by excessive muscularity or obesity on the one hand, or transformed to uncomfortable tenderness by excessive thinness on the other.
Armpits:
Some consider the armpits to be an erogenous zone, despite the similarity of the axillae (armpits) to normal-haired skin in both the density of nerves and hair follicles. Exaggerated or anticipated digital (fingers, toes) or oral (mouth, lips, tongue) stimulation is believed to be responsible for the heightened sensual response.
If pheromones exist for humans, they would likely be secreted by a mixture of liquid from the apocrine glands with other organic compounds in the body.
George Preti, an organic chemist at the Monell Chemical Senses Center in Philadelphia and Winnefred Cutler of the University of Pennsylvania's psychology department, discovered that women with irregular menstrual cycles became regular when exposed to male underarm extracts.
They hypothesized that the only explanation was that underarms contain pheromones, as there was no other explanation for the effects, which mirrored how pheromones affect other mammals.
Fingers:
The fingertips have many nerves and are responsive to very light touches, like the brushing of a tongue, light fingernail scratching or teeth stroking. The sides of the fingers are somewhat less sensitive and more ticklish. Both light and firmer touches work well at the junction of the fingers.
Human fingertips are the second-most sensitive parts of the body, after the tongue.
Legs:
The thighs can be sensitive to touch. An exaggerated tickle on the back of the legs and knees can also be sensitive for some.
Feet and toes:
See also: Foot fetishism
Because of the concentration of nerve endings in the sole and digits of the human foot—and possibly due to the close proximity between the area of the brain dealing with tactile sensations from the feet and the area dealing with sensations from the genitals—the sensations produced by both the licking of the feet and sucking of toes can be pleasurable to some people.
Similarly, massaging the sole of the foot can also produce stimulation. Many people are extremely ticklish in the foot area, especially on the soles.
See also:
Erogenous zones are located all over the human body, but the sensitivity of each varies, and depends on concentrations of nerve endings that can provide pleasurable sensations when stimulated. The touching of another person's erogenous zone is regarded as an act of physical intimacy.
Whether a person finds stimulation in these areas to be pleasurable or objectionable depends on a range of factors, including their level of arousal, the circumstances in which it takes place, the cultural context, the nature of the relationship between the partners, and the partners' personal histories.
Erogenous zones may be classified by the type of sexual response that they generate. Many people are gently aroused when their eyelids, eyebrows, temples, shoulders, hands, arms, and hair are subtly touched.
Gently touching or stroking of these zones stimulates a partner during foreplay and increases the arousal level. Also, the gentle massage or stroke of the abdominal area along with kissing or simply touching the navel can be a type of stimulation.
Classification:
Specific zones:
Specific zones are associated with sexual response, and include the lips and nipples in addition to areas of the genitals, notably corona of the glans penis, clitoris and rest of the vulva, and perianal skin.
These zones have a high density of innervation, and may have an efficiency of wound healing and a capacity to stimulate generalized cerebral arousal.
Nonspecific zones:
In these zones, the skin is similar to normal-haired skin and has the normal high density of nerves and hair follicles. These areas include the sides and back of the neck, the inner arms, the axillae (armpits) and sides of the thorax (chest).
Genitals:
Male:
Males can be aroused by stimulation to the sides of the glans and penis, upper side of the glans, the front side of the scrotum, the skin between the scrotum and anus perineum, and around the anus.
Female:
Parts of the vulva, especially the clitoris, are erogenous zones. While the vagina is not especially sensitive as a whole, its lower third (the area close to the entrance) has concentrations of the nerve endings that can provide pleasurable sensations during sexual activity when stimulated; this is also called the anterior wall of the vagina or the outer one-third of the vagina, and it contains the majority of the vaginal nerve endings, making it more sensitive to touch than the inner two-thirds of the vaginal barrel.
Within the anterior wall of the vagina, there is a patch of ribbed rough tissue which has a texture that is sometimes described as similar to the palate (the roof of a mouth) or a raspberry, and may feel spongy when a woman is sexually aroused.
This is the urethral sponge, which may also be the location of an area that some women report is an erogenous zone; this is sometimes called the G-spot. When stimulated, it may lead to sexual arousal, an orgasm, or female ejaculation.
The existence of the G-spot and whether or not it is a distinct structure is debated among researchers, as reports of its location vary from woman to woman, it appears to be nonexistent in some women, and scientists commonly believe that it is an extension of the clitoris.
Head:
Mouth:
The lips and tongue are sensitive and can be stimulated by kissing and licking. Biting at the lip can also provide stimulus.
Neck:
The neck, clavicle area and the back of the neck are very sensitive, and can be stimulated by licking, kissing or light caressing. Some people also like being bitten gently in these areas, often to the point that a "hickey", or "love-bite" is formed.
Ears:
Some people find whispering or breathing softly in the ear to be pleasurable and relaxing, as well as licking, biting, caressing and/or kissing it especially the area of and behind the earlobe.
Torso:
Chest:
The areola and nipple contain Golgi-Mazzoni, Vater-Pacini and genital corpuscles. No Meissner's corpuscles and few organized nerve endings are present. There are concentrations of nerve tissue in the area of ducts and masses of smooth muscle.
The hair surrounding the areola adds additional sensory tissue. The mass of smooth muscle and glandular-duct tissue in the nipple and areola block the development of normal dermal nerve networks which are present in other erogenous regions and the development of special end organs.
The entire breast has a network of nerve endings, and it has the same number of nerve endings no matter how large the breast is, so that larger breasts may need more stimulation than smaller ones.
Intense nipple stimulation may result in a surge in the production of oxytocin and prolactin which could have a significant effect on the individual's genitals, even to the point that some people of both sexes can achieve orgasm through nipple stimulation alone.
Having the chest, breasts and nipples stimulated manually (hands), digitally (fingers, toes) and/or orally (mouth, lips, teeth, tongue) is a pleasurable experience for many people of both sexes.
Abdomen and navel:
Main articles: Navel fetishism and Alvinolagnia.
Many people find stimulation (kissing, biting, scratching, tickling, caressing) of the abdomen to be pleasurable, especially close to the pubic region. It can cause strong arousal in men and women, in some even stronger than stimulation of the genitals. The navel is one of the many erogenous zones that has heightened sensitivity.
In a 1982 study of eroticism in dress entitled "Skin to Skin", Prudence Glynn claimed that the waist symbolized virginity and that it was the first place that a man would touch a woman "when indicating more than a formal courtesy".
The navel and the region below when touched by the finger or the tip of the tongue result in the production of erotic sensations.
Arms:
The skin of the arms, and specifically the softer skin of the inner arms and across the creased mid-arm bend covering the ventral side of the elbow, are highly sensitive to manual or oral stimulation.
Caressing with fingers or tongue, more vigorous kneading, and butterfly kissing can initiate arousal and, in some cases, induce clitoral/vaginal orgasm or penile ejaculation without direct contact with the latter areas.
The mid-arm bend is especially sensitive due to the thinner skin found there, which makes nerve endings more accessible. Arm sensitivity may be reduced or concentrated to a more narrow range by excessive muscularity or obesity on the one hand, or transformed to uncomfortable tenderness by excessive thinness on the other.
Armpits:
Some consider the armpits to be an erogenous zone, despite the similarity of the axillae (armpits) to normal-haired skin in both the density of nerves and hair follicles. Exaggerated or anticipated digital (fingers, toes) or oral (mouth, lips, tongue) stimulation is believed to be responsible for the heightened sensual response.
If pheromones exist for humans, they would likely be secreted by a mixture of liquid from the apocrine glands with other organic compounds in the body.
George Preti, an organic chemist at the Monell Chemical Senses Center in Philadelphia and Winnefred Cutler of the University of Pennsylvania's psychology department, discovered that women with irregular menstrual cycles became regular when exposed to male underarm extracts.
They hypothesized that the only explanation was that underarms contain pheromones, as there was no other explanation for the effects, which mirrored how pheromones affect other mammals.
Fingers:
The fingertips have many nerves and are responsive to very light touches, like the brushing of a tongue, light fingernail scratching or teeth stroking. The sides of the fingers are somewhat less sensitive and more ticklish. Both light and firmer touches work well at the junction of the fingers.
Human fingertips are the second-most sensitive parts of the body, after the tongue.
Legs:
The thighs can be sensitive to touch. An exaggerated tickle on the back of the legs and knees can also be sensitive for some.
Feet and toes:
See also: Foot fetishism
Because of the concentration of nerve endings in the sole and digits of the human foot—and possibly due to the close proximity between the area of the brain dealing with tactile sensations from the feet and the area dealing with sensations from the genitals—the sensations produced by both the licking of the feet and sucking of toes can be pleasurable to some people.
Similarly, massaging the sole of the foot can also produce stimulation. Many people are extremely ticklish in the foot area, especially on the soles.
See also:
HIV/AIDS InfectionsPictured below: Examples of Symptoms of HIV/Aids
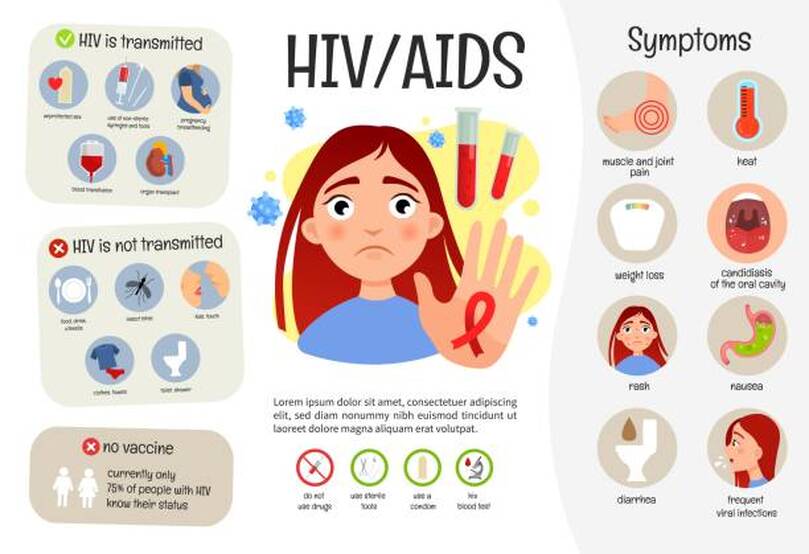
Human immunodeficiency virus infection and acquired immunodeficiency syndrome (HIV/AIDS) is a spectrum of conditions caused by infection with the human immunodeficiency virus (HIV), a retrovirus.
Following initial infection an individual may not notice any symptoms, or may experience a brief period of influenza-like illness. Typically, this is followed by a prolonged incubation period with no symptoms.
If the infection progresses, it interferes more with the immune system, increasing the risk of developing common infections such as tuberculosis, as well as other opportunistic infections, and tumors which are rare in people who have normal immune function. These late symptoms of infection are referred to as acquired immunodeficiency syndrome (AIDS). This stage is often also associated with unintended weight loss.
HIV is spread primarily by unprotected sex (including anal and vaginal sex), contaminated hypodermic needles or blood transfusions, and from mother to child during pregnancy, delivery, or breastfeeding. Some bodily fluids, such as saliva, sweat and tears, do not transmit the virus.
Oral sex has little to no risk of transmitting the virus. Methods of prevention include:
Disease in a baby can often be prevented by giving both the mother and child antiretroviral medication.
Recognized worldwide in the early 1980s, HIV/AIDS has had a large impact on society, both as an illness and as a source of discrimination. The disease also has large economic impacts. There are many misconceptions about HIV/AIDS, such as the belief that it can be transmitted by casual non-sexual contact.
The disease has become subject to many controversies involving religion, including the Catholic Church's position not to support condom use as prevention. It has attracted international medical and political attention as well as large-scale funding since it was identified in the 1980s.
HIV made the jump from other primates to humans in west-central Africa in the early-to-mid 20th century. AIDS was first recognized by the U.S. Centers for Disease Control and Prevention (CDC) in 1981 and its cause—HIV infection—was identified in the early part of the decade.
Between the first time AIDS was readily identified through 2021, the disease is estimated to have caused at least 40 million deaths worldwide. In 2021, there were 650,000 deaths and about 38 million people worldwide living with HIV. An estimated 20.6 million of these people live in eastern and southern Africa. HIV/AIDS is considered a pandemic—a disease outbreak which is present over a large area and is actively spreading.
The United States' National Institutes of Health (NIH) and the Gates Foundation have pledged $200 million focused on developing a global cure for AIDS. While there is no broadly available cure or vaccine, antiretroviral treatment can slow the course of the disease and may lead to a near-normal life expectancy. Treatment is recommended as soon as the diagnosis is made.
Without treatment, the average survival time after infection is 11 years.
Signs and symptoms
Main article: Signs and symptoms of HIV/AIDS
There are three main stages of HIV infection:
Acute infection:
The initial period following the contraction of HIV is called acute HIV, primary HIV or acute retroviral syndrome. Many individuals develop an influenza-like illness or a mononucleosis-like illness 2–4 weeks after exposure while others have no significant symptoms.
Symptoms occur in 40–90% of cases and most commonly include:
The rash, which occurs in 20–50% of cases, presents itself on the trunk and is maculopapular, classically.
Some people also develop opportunistic infections at this stage. Gastrointestinal symptoms, such as vomiting or diarrhea may occur. Neurological symptoms of peripheral neuropathy or Guillain–Barré syndrome also occur. The duration of the symptoms varies, but is usually one or two weeks.
Owing to their nonspecific character, these symptoms are not often recognized as signs of HIV infection. Even cases that do get seen by a family doctor or a hospital are often misdiagnosed as one of the many common infectious diseases with overlapping symptoms.
Thus, it is recommended that HIV be considered in people presenting with an unexplained fever who may have risk factors for the infection.
Clinical latency:
The initial symptoms are followed by a stage called clinical latency, asymptomatic HIV, or chronic HIV. Without treatment, this second stage of the natural history of HIV infection can last from about three years to over 20 years (on average, about eight years).
While typically there are few or no symptoms at first, near the end of this stage many people experience fever, weight loss, gastrointestinal problems and muscle pains. Between 50% and 70% of people also develop persistent generalized lymphadenopathy, characterized by unexplained, non-painful enlargement of more than one group of lymph nodes (other than in the groin) for over three to six months.
Although most HIV-1 infected individuals have a detectable viral load and in the absence of treatment will eventually progress to AIDS, a small proportion (about 5%) retain high levels of CD4+ T cells (T helper cells) without antiretroviral therapy for more than five years.
These individuals are classified as "HIV controllers" or long-term nonprogressors (LTNP). Another group consists of those who maintain a low or undetectable viral load without anti-retroviral treatment, known as "elite controllers" or "elite suppressors". They represent approximately 1 in 300 infected persons.
Acquired immunodeficiency syndrome:
Acquired immunodeficiency syndrome (AIDS) is defined as an HIV infection with either a CD4+ T cell count below 200 cells per µL or the occurrence of specific diseases associated with HIV infection. In the absence of specific treatment, around half of people infected with HIV develop AIDS within ten years.
The most common initial conditions that alert to the presence of AIDS are pneumocystis pneumonia (40%), cachexia in the form of HIV wasting syndrome (20%), and esophageal candidiasis. Other common signs include recurrent respiratory tract infections.
Opportunistic infections may be caused by bacteria, viruses, fungi, and parasites that are normally controlled by the immune system. Which infections occur depends partly on what organisms are common in the person's environment. These infections may affect nearly every organ system.
People with AIDS have an increased risk of developing various viral-induced cancers, including:
Kaposi's sarcoma is the most common cancer, occurring in 10% to 20% of people with HIV. The second-most common cancer is lymphoma, which is the cause of death of nearly 16% of people with AIDS and is the initial sign of AIDS in 3% to 4%. Both these cancers are associated with human herpesvirus 8 (HHV-8). Cervical cancer occurs more frequently in those with AIDS because of its association with human papillomavirus (HPV).
Conjunctival cancer (of the layer that lines the inner part of eyelids and the white part of the eye) is also more common in those with HIV.
Additionally, people with AIDS frequently have systemic symptoms such as prolonged fevers, sweats (particularly at night), swollen lymph nodes, chills, weakness, and unintended weight loss. Diarrhea is another common symptom, present in about 90% of people with AIDS. They can also be affected by diverse psychiatric and neurological symptoms independent of opportunistic infections and cancers.
Transmission
HIV is spread by three main routes: sexual contact, significant exposure to infected body fluids or tissues, and from mother to child during pregnancy, delivery, or breastfeeding (known as vertical transmission).
There is no risk of acquiring HIV if exposed to feces, nasal secretions, saliva, sputum, sweat, tears, urine, or vomit unless these are contaminated with blood. It is also possible to be co-infected by more than one strain of HIV—a condition known as HIV superinfection.
Sexual:
The most frequent mode of transmission of HIV is through sexual contact with an infected person. However, an HIV-positive person who has an undetectable viral load as a result of long-term treatment has effectively no risk of transmitting HIV sexually.
The existence of functionally noncontagious HIV-positive people on antiretroviral therapy was controversially publicized in the 2008 Swiss Statement, and has since become accepted as medically sound.
Globally, the most common mode of HIV transmission is via sexual contacts between people of the opposite sex; however, the pattern of transmission varies among countries. As of 2017, most HIV transmission in the United States occurred among men who had sex with men (82% of new HIV diagnoses among males aged 13 and older and 70% of total new diagnoses).
In the US, gay and bisexual men aged 13 to 24 accounted for an estimated 92% of new HIV diagnoses among all men in their age group and 27% of new diagnoses among all gay and bisexual men.
With regard to unprotected heterosexual contacts, estimates of the risk of HIV transmission per sexual act appear to be four to ten times higher in low-income countries than in high-income countries.
In low-income countries, the risk of female-to-male transmission is estimated as 0.38% per act, and of male-to-female transmission as 0.30% per act; the equivalent estimates for high-income countries are 0.04% per act for female-to-male transmission, and 0.08% per act for male-to-female transmission.
The risk of transmission from anal intercourse is especially high, estimated as 1.4–1.7% per act in both heterosexual and homosexual contacts. While the risk of transmission from oral sex is relatively low, it is still present. The risk from receiving oral sex has been described as "nearly nil"; however, a few cases have been reported. The per-act risk is estimated at 0–0.04% for receptive oral intercourse.
In settings involving prostitution in low-income countries, risk of female-to-male transmission has been estimated as 2.4% per act, and of male-to-female transmission as 0.05% per act.
Risk of transmission increases in the presence of many sexually transmitted infections and genital ulcers. Genital ulcers appear to increase the risk approximately fivefold.
Other sexually transmitted infections, such as gonorrhea, chlamydia, trichomoniasis, and bacterial vaginosis, are associated with somewhat smaller increases in risk of transmission.
The viral load of an infected person is an important risk factor in both sexual and mother-to-child transmission. During the first 2.5 months of an HIV infection a person's infectiousness is twelve times higher due to the high viral load associated with acute HIV.
If the person is in the late stages of infection, rates of transmission are approximately eightfold greater.
Commercial sex workers (including those in pornography) have an increased likelihood of contracting HIV. Rough sex can be a factor associated with an increased risk of transmission.
Sexual assault is also believed to carry an increased risk of HIV transmission as condoms are rarely worn, physical trauma to the vagina or rectum is likely, and there may be a greater risk of concurrent sexually transmitted infections.
Body fluids:
The second-most frequent mode of HIV transmission is via blood and blood products. Blood-borne transmission can be through needle-sharing during intravenous drug use, needle-stick injury, transfusion of contaminated blood or blood product, or medical injections with unsterilized equipment.
The risk from sharing a needle during drug injection is between 0.63% and 2.4% per act, with an average of 0.8%. The risk of acquiring HIV from a needle stick from an HIV-infected person is estimated as 0.3% (about 1 in 333) per act and the risk following mucous membrane exposure to infected blood as 0.09% (about 1 in 1000) per act.
This risk may, however, can be up to 5% if the introduced blood was from a person with a high viral load and the cut was deep. In the United States, intravenous drug users made up 12% of all new cases of HIV in 2009, and in some areas more than 80% of people who inject drugs are HIV-positive.
HIV is transmitted in about 90% of blood transfusions using infected blood. In developed countries the risk of acquiring HIV from a blood transfusion is extremely low (less than one in half a million) where improved donor selection and HIV screening is performed; for example, in the UK the risk is reported at one in five million and in the United States it was one in 1.5 million in 2008.
In low-income countries, only half of transfusions may be appropriately screened (as of 2008), and it is estimated that up to 15% of HIV infections in these areas come from transfusion of infected blood and blood products, representing between 5% and 10% of global infections.
It is possible to acquire HIV from organ and tissue transplantation, although this is rare because of screening.
Unsafe medical injections play a role in HIV spread in sub-Saharan Africa. In 2007, between 12% and 17% of infections in this region were attributed to medical syringe use.
The World Health Organization estimates the risk of transmission as a result of a medical injection in Africa at 1.2%. Risks are also associated with invasive procedures, assisted delivery, and dental care in this area of the world.
People giving or receiving tattoos, piercings, and scarification are theoretically at risk of infection but no confirmed cases have been documented. It is not possible for mosquitoes or other insects to transmit HIV.
Mother-to-child:
Main articles:
HIV can be transmitted from mother to child during pregnancy, during delivery, or through breast milk, resulting in the baby also contracting HIV.
As of 2008, vertical transmission accounted for about 90% of cases of HIV in children. In the absence of treatment, the risk of transmission before or during birth is around 20%, and in those who also breastfeed 35%. Treatment can decrease this risk to less than 5%.
Antiretrovirals when taken by either the mother or the baby decrease the risk of transmission in those who do breastfeed. If blood contaminates food during pre-chewing it may pose a risk of transmission.
If a woman is untreated, two years of breastfeeding results in an HIV/AIDS risk in her baby of about 17%. Due to the increased risk of death without breastfeeding in many areas in the developing world, the World Health Organization recommends either exclusive breastfeeding or the provision of safe formula.
All women known to be HIV-positive should be taking lifelong antiretroviral therapy.
Virology:
Main article: HIV
HIV is the cause of the spectrum of disease known as HIV/AIDS. HIV is a retrovirus that primarily infects components of the human immune system such as CD4+ T cells, macrophages and dendritic cells. It directly and indirectly destroys CD4+ T cells.
HIV is a member of the genus Lentivirus, part of the family Retroviridae. Lentiviruses share many morphological and biological characteristics. Many species of mammals are infected by lentiviruses, which are characteristically responsible for long-duration illnesses with a long incubation period.
Lentiviruses are transmitted as single-stranded, positive-sense, enveloped RNA viruses. Upon entry into the target cell, the viral RNA genome is converted (reverse transcribed) into double-stranded DNA by a virally encoded reverse transcriptase that is transported along with the viral genome in the virus particle.
The resulting viral DNA is then imported into the cell nucleus and integrated into the cellular DNA by a virally encoded integrase and host co-factors. Once integrated, the virus may become latent, allowing the virus and its host cell to avoid detection by the immune system.
Alternatively, the virus may be transcribed, producing new RNA genomes and viral proteins that are packaged and released from the cell as new virus particles that begin the replication cycle anew.
HIV is now known to spread between CD4+ T cells by two parallel routes: cell-free spread and cell-to-cell spread, i.e. it employs hybrid spreading mechanisms. In the cell-free spread, virus particles bud from an infected T cell, enter the blood/extracellular fluid and then infect another T cell following a chance encounter.
HIV can also disseminate by direct transmission from one cell to another by a process of cell-to-cell spread. The hybrid spreading mechanisms of HIV contribute to the virus's ongoing replication against antiretroviral therapies.
Two types of HIV have been characterized: HIV-1 and HIV-2. HIV-1 is the virus that was originally discovered (and initially referred to also as LAV or HTLV-III). It is more virulent, more infective, and is the cause of the majority of HIV infections globally. The lower infectivity of HIV-2 as compared with HIV-1 implies that fewer people exposed to HIV-2 will be infected per exposure.
Because of its relatively poor capacity for transmission, HIV-2 is largely confined to West Africa.
Pathophysiology:
Main article: Pathophysiology of HIV/AIDS
2
After the virus enters the body, there is a period of rapid viral replication, leading to an abundance of virus in the peripheral blood. During primary infection, the level of HIV may reach several million virus particles per milliliter of blood. This response is accompanied by a marked drop in the number of circulating CD4+ T cells.
The acute viremia is almost invariably associated with activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts recover. A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus.
Ultimately, HIV causes AIDS by depleting CD4+ T cells. This weakens the immune system and allows opportunistic infections. T cells are essential to the immune response and without them, the body cannot fight infections or kill cancerous cells.
The mechanism of CD4+ T cell depletion differs in the acute and chronic phases. During the acute phase, HIV-induced cell lysis and killing of infected cells by CD8+ T cells accounts for CD4+ T cell depletion, although apoptosis may also be a factor.
During the chronic phase, the consequences of generalized immune activation coupled with the gradual loss of the ability of the immune system to generate new T cells appear to account for the slow decline in CD4+ T cell numbers.
Although the symptoms of immune deficiency characteristic of AIDS do not appear for years after a person is infected, the bulk of CD4+ T cell loss occurs during the first weeks of infection, especially in the intestinal mucosa, which harbors the majority of the lymphocytes found in the body.
The reason for the preferential loss of mucosal CD4+ T cells is that the majority of mucosal CD4+ T cells express the CCR5 protein which HIV uses as a co-receptor to gain access to the cells, whereas only a small fraction of CD4+ T cells in the bloodstream do so.
A specific genetic change that alters the CCR5 protein when present in both chromosomes very effectively prevents HIV-1 infection.
HIV seeks out and destroys CCR5 expressing CD4+ T cells during acute infection. A vigorous immune response eventually controls the infection and initiates the clinically latent phase. CD4+ T cells in mucosal tissues remain particularly affected.
Continuous HIV replication causes a state of generalized immune activation persisting throughout the chronic phase. Immune activation, which is reflected by the increased activation state of immune cells and release of pro-inflammatory cytokines, results from the activity of several HIV gene products and the immune response to ongoing HIV replication.
It is also linked to the breakdown of the immune surveillance system of the gastrointestinal mucosal barrier caused by the depletion of mucosal CD4+ T cells during the acute phase of disease.
Diagnosis:
Main article: Diagnosis of HIV/AIDS
HIV/AIDS is diagnosed via laboratory testing and then staged based on the presence of certain signs or symptoms. HIV screening is recommended by the United States Preventive Services Task Force for all people 15 years to 65 years of age, including all pregnant women.
Additionally, testing is recommended for those at high risk, which includes anyone diagnosed with a sexually transmitted illness. In many areas of the world, a third of HIV carriers only discover they are infected at an advanced stage of the disease when AIDS or severe immunodeficiency has become apparent.
HIV testing:
Most people infected with HIV develop specific antibodies (i.e. seroconvert) within three to twelve weeks after the initial infection. Diagnosis of primary HIV before seroconversion is done by measuring HIV-RNA or p24 antigen. Positive results obtained by antibody or PCR testing are confirmed either by a different antibody or by PCR.
Antibody tests in children younger than 18 months are typically inaccurate, due to the continued presence of maternal antibodies. Thus HIV infection can only be diagnosed by PCR testing for HIV RNA or DNA, or via testing for the p24 antigen. Much of the world lacks access to reliable PCR testing, and people in many places simply wait until either symptoms develop or the child is old enough for accurate antibody testing.
In sub-Saharan Africa between 2007 and 2009, between 30% and 70% of the population were aware of their HIV status. In 2009, between 3.6% and 42% of men and women in sub-Saharan countries were tested; this represented a significant increase compared to previous years.
Classifications:
Two main clinical staging systems are used to classify HIV and HIV-related disease for surveillance purposes: the WHO disease staging system for HIV infection and disease, and the CDC classification system for HIV infection. The CDC's classification system is more frequently adopted in developed countries.
Since the WHO's staging system does not require laboratory tests, it is suited to the resource-restricted conditions encountered in developing countries, where it can also be used to help guide clinical management. Despite their differences, the two systems allow a comparison for statistical purposes.
The World Health Organization first proposed a definition for AIDS in 1986. Since then, the WHO classification has been updated and expanded several times, with the most recent version being published in 2007.
The WHO system uses the following categories:
The U.S. Centers for Disease Control and Prevention also created a classification system for HIV, and updated it in 2008 and 2014. This system classifies HIV infections based on CD4 count and clinical symptoms, and describes the infection in five groups. In those greater than six years of age it is:
For surveillance purposes, the AIDS diagnosis still stands even if, after treatment, the CD4+ T cell count rises to above 200 per µL of blood or other AIDS-defining illnesses are cured.
Prevention:
Main article: Prevention of HIV/AIDS
Sexual Contact:
Consistent condom use reduces the risk of HIV transmission by approximately 80% over the long term. When condoms are used consistently by a couple in which one person is infected, the rate of HIV infection is less than 1% per year.
There is some evidence to suggest that female condoms may provide an equivalent level of protection.
Application of a vaginal gel containing tenofovir (a reverse transcriptase inhibitor) immediately before sex seems to reduce infection rates by approximately 40% among African women.
By contrast, use of the spermicide nonoxynol-9 may increase the risk of transmission due to its tendency to cause vaginal and rectal irritation.
Circumcision in sub-Saharan Africa "reduces the acquisition of HIV by heterosexual men by between 38% and 66% over 24 months". Owing to these studies, both the World Health Organization and UNAIDS recommended male circumcision in 2007 as a method of preventing female-to-male HIV transmission in areas with high rates of HIV.
However, whether it protects against male-to-female transmission is disputed, and whether it is of benefit in developed countries and among men who have sex with men is undetermined.
Programs encouraging sexual abstinence do not appear to affect subsequent HIV risk.
Evidence of any benefit from peer education is equally poor. Comprehensive sexual education provided at school may decrease high-risk behavior.
A substantial minority of young people continues to engage in high-risk practices despite knowing about HIV/AIDS, underestimating their own risk of becoming infected with HIV.
Voluntary counseling and testing people for HIV does not affect risky behavior in those who test negative but does increase condom use in those who test positive. Enhanced family planning services appear to increase the likelihood of women with HIV using contraception, compared to basic services. It is not known whether treating other sexually transmitted infections is effective in preventing HIV.
Pre-exposure:
Antiretroviral treatment among people with HIV whose CD4 count ≤ 550 cells/µL is a very effective way to prevent HIV infection of their partner (a strategy known as treatment as prevention, or TASP). TASP is associated with a 10- to 20-fold reduction in transmission risk.
Pre-exposure prophylaxis (PrEP) with a daily dose of the medications tenofovir, with or without emtricitabine, is effective in people at high risk including men who have sex with men, couples where one is HIV-positive, and young heterosexuals in Africa. It may also be effective in intravenous drug users, with a study finding a decrease in risk of 0.7 to 0.4 per 100 person years. The USPSTF, in 2019, recommended PrEP in those who are at high risk.
Universal precautions within the health care environment are believed to be effective in decreasing the risk of HIV. Intravenous drug use is an important risk factor, and harm reduction strategies such as needle-exchange programs and opioid substitution therapy appear effective in decreasing this risk.
Post-exposure:
A course of antiretrovirals administered within 48 to 72 hours after exposure to HIV-positive blood or genital secretions is referred to as post-exposure prophylaxis (PEP). The use of the single agent zidovudine reduces the risk of a HIV infection five-fold following a needle-stick injury.
As of 2013, the prevention regimen recommended in the United States consists of three medications--tenofovir, emtricitabine and raltegravir—as this may reduce the risk further.
PEP treatment is recommended after a sexual assault when the perpetrator is known to be HIV-positive, but is controversial when their HIV status is unknown. The duration of treatment is usually four weeks and is frequently associated with adverse effects—where zidovudine is used, about 70% of cases result in adverse effects such as nausea (24%), fatigue (22%), emotional distress (13%) and headaches (9%).
Mother-to-child:
Main article: HIV and pregnancy
Programs to prevent the vertical transmission of HIV (from mothers to children) can reduce rates of transmission by 92–99%. This primarily involves the use of a combination of antiviral medications during pregnancy and after birth in the infant, and potentially includes bottle feeding rather than breastfeeding.
If replacement feeding is acceptable, feasible, affordable, sustainable and safe, mothers should avoid breastfeeding their infants; however, exclusive breastfeeding is recommended during the first months of life if this is not the case. If exclusive breastfeeding is carried out, the provision of extended antiretroviral prophylaxis to the infant decreases the risk of transmission.
In 2015, Cuba became the first country in the world to eradicate mother-to-child transmission of HIV.
Vaccination:
Main article: HIV vaccine
Currently there is no licensed vaccine for HIV or AIDS.The most effective vaccine trial to date, RV 144, was published in 2009; it found a partial reduction in the risk of transmission of roughly 30%, stimulating some hope in the research community of developing a truly effective vaccine.
Treatment:
Main article: Management of HIV/AIDS
There is currently no cure, nor an effective HIV vaccine. Treatment consists of highly active antiretroviral therapy (HAART), which slows progression of the disease. As of 2010, more than 6.6 million people were receiving HAART in low- and middle-income countries.
Treatment also includes preventive and active treatment of opportunistic infections. As of July 2022, four people have been successfully cleared of HIV. Rapid initiation of antiretroviral therapy within one week of diagnosis appear to improve treatment outcomes in low and medium-income settings.
Antiviral therapy:
Current HAART options are combinations (or "cocktails") consisting of at least three medications belonging to at least two types, or "classes", of antiretroviral agents.
Initially, treatment is typically a non-nucleoside reverse transcriptase inhibitor (NNRTI) plus two nucleoside analog reverse transcriptase inhibitors (NRTIs). Typical NRTIs include: zidovudine (AZT) or tenofovir (TDF) and lamivudine (3TC) or emtricitabine (FTC).
As of 2019, dolutegravir/lamivudine/tenofovir is listed by the World Health Organization as the first-line treatment for adults, with tenofovir/lamivudine/efavirenz as an alternative.
Combinations of agents that include protease inhibitors (PI) are used if the above regimen loses effectiveness.
The World Health Organization and the United States recommend antiretrovirals in people of all ages (including pregnant women) as soon as the diagnosis is made, regardless of CD4 count. Once treatment is begun, it is recommended that it is continued without breaks or "holidays".
Many people are diagnosed only after treatment ideally should have begun. The desired outcome of treatment is a long-term plasma HIV-RNA count below 50 copies/mL. Levels to determine if treatment is effective are initially recommended after four weeks and once levels fall below 50 copies/mL checks every three to six months are typically adequate.
Inadequate control is deemed to be greater than 400 copies/mL. Based on these criteria treatment is effective in more than 95% of people during the first year.
Benefits of treatment include a decreased risk of progression to AIDS and a decreased risk of death. In the developing world, treatment also improves physical and mental health.
With treatment, there is a 70% reduced risk of acquiring tuberculosis. Additional benefits include a decreased risk of transmission of the disease to sexual partners and a decrease in mother-to-child transmission.
The effectiveness of treatment depends to a large part on compliance. Reasons for non-adherence to treatment include poor access to medical care, inadequate social supports, mental illness and drug abuse. The complexity of treatment regimens (due to pill numbers and dosing frequency) and adverse effects may reduce adherence.
Even though cost is an important issue with some medications, 47% of those who needed them were taking them in low- and middle-income countries as of 2010, and the rate of adherence is similar in low-income and high-income countries.
Specific adverse events are related to the antiretroviral agent taken. Some relatively common adverse events include: lipodystrophy syndrome, dyslipidemia, and diabetes mellitus, especially with protease inhibitors.
Other common symptoms include diarrhea, and an increased risk of cardiovascular disease. Newer recommended treatments are associated with fewer adverse effects. Certain medications may be associated with birth defects and therefore may be unsuitable for women hoping to have children.
Treatment recommendations for children are somewhat different from those for adults. The World Health Organization recommends treating all children less than five years of age; children above five are treated like adults.
The United States guidelines recommend treating all children less than 12 months of age and all those with HIV RNA counts greater than 100,000 copies/mL between one year and five years of age.
The European Medicines Agency (EMA) has recommended the granting of marketing authorizations for two new antiretroviral (ARV) medicines, rilpivirine (Rekambys) and cabotegravir (Vocabria), to be used together for the treatment of people with human immunodeficiency virus type 1 (HIV-1) infection.
The two medicines are the first ARVs that come in a long-acting injectable formulation. This means that instead of daily pills, people receive intramuscular injections monthly or every two months.
The combination of Rekambys and Vocabria injection is intended for maintenance treatment of adults who have undetectable HIV levels in the blood (viral load less than 50 copies/ml) with their current ARV treatment, and when the virus has not developed resistance to a certain class of anti-HIV medicines called non-nucleoside reverse transcriptase inhibitors (NNRTIs) and integrase strand transfer inhibitors (INIs).
Cabotegravir combined with rilpivirine (Cabenuva) is a complete regimen for the treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults to replace a current antiretroviral regimen in those who are virologically suppressed on a stable antiretroviral regimen with no history of treatment failure and with no known or suspected resistance to either cabotegravir or rilpivirine.
Opportunistic infections:
Main article: Opportunistic infection § Opportunistic Infection and HIV/AIDS
Measures to prevent opportunistic infections are effective in many people with HIV/AIDS. In addition to improving current disease, treatment with antiretrovirals reduces the risk of developing additional opportunistic infections.
Adults and adolescents who are living with HIV (even on anti-retroviral therapy) with no evidence of active tuberculosis in settings with high tuberculosis burden should receive isoniazid preventive therapy (IPT); the tuberculin skin test can be used to help decide if IPT is needed.
Children with HIV may benefit from screening for tuberculosis.
Vaccination against hepatitis A and B is advised for all people at risk of HIV before they become infected; however, it may also be given after infection.
Trimethoprim/sulfamethoxazole prophylaxis between four and six weeks of age, and ceasing breastfeeding of infants born to HIV-positive mothers, is recommended in resource-limited settings. It is also recommended to prevent PCP when a person's CD4 count is below 200 cells/uL and in those who have or have previously had PCP.
People with substantial immunosuppression are also advised to receive prophylactic therapy for toxoplasmosis and MAC. Appropriate preventive measures reduced the rate of these infections by 50% between 1992 and 1997. Influenza vaccination and pneumococcal polysaccharide vaccine are often recommended in people with HIV/AIDS with some evidence of benefit.
Diet:
Main article: Nutrition and HIV/AIDS
The World Health Organization (WHO) has issued recommendations regarding nutrient requirements in HIV/AIDS. A generally healthy diet is promoted. Dietary intake of micronutrients at RDA levels by HIV-infected adults is recommended by the WHO; higher intake of vitamin A, zinc, and iron can produce adverse effects in HIV-positive adults, and is not recommended unless there is documented deficiency.
Dietary supplementation for people who are infected with HIV and who have inadequate nutrition or dietary deficiencies may strengthen their immune systems or help them recover from infections; however, evidence indicating an overall benefit in morbidity or reduction in mortality is not consistent.
People with HIV/AIDS are up to four times more likely to develop type 2 diabetes than those who are not tested positive with the virus.
Evidence for supplementation with selenium is mixed with some tentative evidence of benefit. For pregnant and lactating women with HIV, multivitamin supplement improves outcomes for both mothers and children. If the pregnant or lactating mother has been advised to take anti-retroviral medication to prevent mother-to-child HIV transmission, multivitamin supplements should not replace these treatments.
There is some evidence that vitamin A supplementation in children with an HIV infection reduces mortality and improves growth.
Alternative medicine:
In the US, approximately 60% of people with HIV use various forms of complementary or alternative medicine, whose effectiveness has not been established. There is not enough evidence to support the use of herbal medicines. There is insufficient evidence to recommend or support the use of medical cannabis to try to increase appetite or weight gain.
Prognosis:
HIV/AIDS has become a chronic rather than an acutely fatal disease in many areas of the world. Prognosis varies between people, and both the CD4 count and viral load are useful for predicted outcomes.
Without treatment, average survival time after infection with HIV is estimated to be 9 to 11 years, depending on the HIV subtype. After the diagnosis of AIDS, if treatment is not available, survival ranges between 6 and 19 months.
HAART and appropriate prevention of opportunistic infections reduces the death rate by 80%, and raises the life expectancy for a newly diagnosed young adult to 20–50 years. This is between two thirds and nearly that of the general population.
If treatment is started late in the infection, prognosis is not as good: for example, if treatment is begun following the diagnosis of AIDS, life expectancy is ~10–40 years. Half of infants born with HIV die before two years of age without treatment.
The primary causes of death from HIV/AIDS are opportunistic infections and cancer, both of which are frequently the result of the progressive failure of the immune system.Risk of cancer appears to increase once the CD4 count is below 500/μL.
The rate of clinical disease progression varies widely between individuals and has been shown to be affected by a number of factors such as:
Tuberculosis co-infection is one of the leading causes of sickness and death in those with HIV/AIDS being present in a third of all HIV-infected people and causing 25% of HIV-related deaths.
HIV is also one of the most important risk factors for tuberculosis. Hepatitis C is another very common co-infection where each disease increases the progression of the other.
The two most common cancers associated with HIV/AIDS are Kaposi's sarcoma and AIDS-related non-Hodgkin's lymphoma. Other cancers that are more frequent include:
Even with anti-retroviral treatment, over the long term HIV-infected people may experience:
Some conditions, such as lipodystrophy, may be caused both by HIV and its treatment.
Epidemiology:
Main article: Epidemiology of HIV/AIDS
Some authors consider HIV/AIDS a global pandemic. As of 2016, approximately 36.7 million people worldwide have HIV, the number of new infections that year being about 1.8 million. This is down from 3.1 million new infections in 2001. Slightly over half the infected population are women and 2.1 million are children. It resulted in about 1 million deaths in 2016, down from a peak of 1.9 million in 2005.
Sub-Saharan Africa is the region most affected. In 2010, an estimated 68% (22.9 million) of all HIV cases and 66% of all deaths (1.2 million) occurred in this region. This means that about 5% of the adult population is infected and it is believed to be the cause of 10% of all deaths in children.
Here, in contrast to other regions, women comprise nearly 60% of cases. South Africa has the largest population of people with HIV of any country in the world at 5.9 million.
Life expectancy has fallen in the worst-affected countries due to HIV/AIDS; for example, in 2006 it was estimated that it had dropped from 65 to 35 years in Botswana. Mother-to-child transmission in Botswana and South Africa, as of 2013, has decreased to less than 5%, with improvement in many other African nations due to improved access to antiretroviral therapy.
South & South East Asia is the second most affected; in 2010 this region contained an estimated 4 million cases or 12% of all people living with HIV resulting in approximately 250,000 deaths. Approximately 2.4 million of these cases are in India.
During 2008 in the United States approximately 1.2 million people aged ≥13 years were living with HIV, resulting in about 17,500 deaths. The US Centers for Disease Control and Prevention estimated that in that year, 236,400 people or 20% of infected Americans were unaware of their infection.
As of 2016 about 675,000 people have died of HIV/AIDS in the US since the beginning of the HIV epidemic. In the United Kingdom as of 2015, there were approximately 101,200 cases which resulted in 594 deaths.
In Canada as of 2008, there were about 65,000 cases causing 53 deaths. Between the first recognition of AIDS (in 1981) and 2009, it has led to nearly 30 million deaths. Rates of HIV are lowest in North Africa and the Middle East (0.1% or less), East Asia (0.1%), and Western and Central Europe (0.2%).
The worst-affected European countries, in 2009 and 2012 estimates, are Russia, Ukraine, Latvia, Moldova, Portugal and Belarus, in decreasing order of prevalence.
History:
Main article: History of HIV/AIDS
Discovery:
The first news story on the disease appeared on May 18, 1981, in the gay newspaper New York Native.
AIDS was first clinically reported on June 5, 1981, with five cases in the United States. The initial cases were a cluster of injecting drug users and gay men with no known cause of impaired immunity who showed symptoms of Pneumocystis carinii pneumonia (PCP), a rare opportunistic infection that was known to occur in people with very compromised immune systems.
Soon thereafter, a large number of homosexual men developed a generally rare skin cancer called Kaposi's sarcoma (KS). Many more cases of PCP and KS emerged, alerting U.S. Centers for Disease Control and Prevention (CDC) and a CDC task force was formed to monitor the outbreak.
In the early days, the CDC did not have an official name for the disease, often referring to it by way of diseases associated with it, such as lymphadenopathy, the disease after which the discoverers of HIV originally named the virus.
They also used Kaposi's sarcoma and opportunistic infections, the name by which a task force had been set up in 1981. At one point the CDC referred to it as the "4H disease", as the syndrome seemed to affect heroin users, homosexuals, hemophiliacs, and Haitians.
The term GRID, which stood for gay-related immune deficiency, had also been coined. However, after determining that AIDS was not isolated to the gay community, it was realized that the term GRID was misleading, and the term AIDS was introduced at a meeting in July 1982.
By September 1982 the CDC started referring to the disease as AIDS.
In 1983, two separate research groups led by Robert Gallo and Luc Montagnier declared that a novel retrovirus may have been infecting people with AIDS, and published their findings in the same issue of the journal Science.
Gallo claimed a virus which his group had isolated from a person with AIDS was strikingly similar in shape to other human T-lymphotropic viruses (HTLVs) that his group had been the first to isolate. Gallo's group called their newly isolated virus HTLV-III.
At the same time, Montagnier's group isolated a virus from a person presenting with swelling of the lymph nodes of the neck and physical weakness, two characteristic symptoms of AIDS.
Contradicting the report from Gallo's group, Montagnier and his colleagues showed that core proteins of this virus were immunologically different from those of HTLV-I. Montagnier's group named their isolated virus lymphadenopathy-associated virus (LAV).
As these two viruses turned out to be the same, in 1986, LAV and HTLV-III were renamed HIV.
Origins:
The origin of HIV / AIDS and the circumstances that led to its emergence remain unsolved.
Both HIV-1 and HIV-2 are believed to have originated in non-human primates in West-central Africa and were transferred to humans in the early 20th century.
HIV-1 appears to have originated in southern Cameroon through the evolution of SIV(cpz), a simian immunodeficiency virus (SIV) that infects wild chimpanzees (HIV-1 descends from the SIVcpz endemic in the chimpanzee subspecies Pan troglodytes troglodytes).
The closest relative of HIV-2 is SIV (smm), a virus of the sooty mangabey (Cercocebus atys atys), an Old World monkey living in coastal West Africa (from southern Senegal to western Ivory Coast).
New World monkeys such as the owl monkey are resistant to HIV-1 infection, possibly because of a genomic fusion of two viral resistance genes. HIV-1 is thought to have jumped the species barrier on at least three separate occasions, giving rise to the three groups of the virus, M, N, and O.
There is evidence that humans who participate in bushmeat activities, either as hunters or as bushmeat vendors, commonly acquire SIV. However, SIV is a weak virus which is typically suppressed by the human immune system within weeks of infection.
It is thought that several transmissions of the virus from individual to individual in quick succession are necessary to allow it enough time to mutate into HIV.
Furthermore, due to its relatively low person-to-person transmission rate, SIV can only spread throughout the population in the presence of one or more high-risk transmission channels, which are thought to have been absent in Africa before the 20th century.
Specific proposed high-risk transmission channels, allowing the virus to adapt to humans and spread throughout society, depend on the proposed timing of the animal-to-human crossing.
Genetic studies of the virus suggest that the most recent common ancestor of the HIV-1 M group dates back to c. 1910. Proponents of this dating link the HIV epidemic with the emergence of colonialism and growth of large colonial African cities, leading to social changes, including a higher degree of sexual promiscuity, the spread of prostitution, and the accompanying high frequency of genital ulcer diseases (such as syphilis) in nascent colonial cities.
While transmission rates of HIV during vaginal intercourse are low under regular circumstances, they are increased manyfold if one of the partners has a sexually transmitted infection causing genital ulcers. Early 1900s colonial cities were notable for their high prevalence of prostitution and genital ulcers, to the degree that, as of 1928, as many as 45% of female residents of eastern Kinshasa were thought to have been prostitutes, and, as of 1933, around 15% of all residents of the same city had syphilis.
An alternative view holds that unsafe medical practices in Africa after World War II, such as unsterile reuse of single-use syringes during mass vaccination, antibiotic and anti-malaria treatment campaigns, were the initial vector that allowed the virus to adapt to humans and spread.
The earliest well-documented case of HIV in a human dates back to 1959 in the Congo. The virus may have been present in the U.S. as early as the mid-to-late 1950s, as a sixteen-year-old male named Robert Rayford presented with symptoms in 1966 and died in 1969. In the 1970s, there were cases of getting parasites and becoming sick with what was called "gay bowel disease", but what is now suspected to have been AIDS.
The earliest retrospectively described case of AIDS is believed to have been in Norway beginning in 1966, that of Arvid Noe. In July 1960, in the wake of Congo's independence, the United Nations recruited Francophone experts and technicians from all over the world to assist in filling administrative gaps left by Belgium, who did not leave behind an African elite to run the country.
By 1962, Haitians made up the second-largest group of well-educated experts (out of the 48 national groups recruited), that totaled around 4500 in the country. Dr. Jacques Pépin, a Canadian author of The Origins of AIDS, stipulates that Haiti was one of HIV's entry points to the U.S. and that a Haitian may have carried HIV back across the Atlantic in the 1960s.
Although there was known to have been at least one case of AIDS in the U.S. from 1966, the vast majority of infections occurring outside sub-Saharan Africa (including the U.S.) can be traced back to a single unknown individual who became infected with HIV in Haiti and brought the infection to the U.S. at some time around 1969. The epidemic rapidly spread among high-risk groups (initially, sexually promiscuous men who have sex with men).
By 1978, the prevalence of HIV-1 among gay male residents of New York City and San Francisco was estimated at 5%, suggesting that several thousand individuals in the country had been infected.
Society and culture
Stigma:
Main article: Discrimination against people with HIV/AIDS
AIDS stigma exists around the world in a variety of ways, including:
Stigma-related violence or the fear of violence prevents many people from seeking HIV testing, returning for their results, or securing treatment, possibly turning what could be a manageable chronic illness into a death sentence and perpetuating the spread of HIV.
AIDS stigma has been further divided into the following three categories:
Often, AIDS stigma is expressed in conjunction with one or more other stigmas, particularly those associated with homosexuality, bisexuality, promiscuity, prostitution, and intravenous drug use.
In many developed countries, there is an association between AIDS and homosexuality or bisexuality, and this association is correlated with higher levels of sexual prejudice, such as anti-homosexual or anti-bisexual attitudes.
There is also a perceived association between AIDS and all male-male sexual behavior, including sex between uninfected men. However, the dominant mode of spread worldwide for HIV remains heterosexual transmission.
To get a better understanding of the anti-homosexual attitudes around AIDs the musical Rent explores this.
In 2003, as part of an overall reform of marriage and population legislation, it became legal for those diagnosed with AIDS to marry in China.
In 2013, the U.S. National Library of Medicine developed a traveling exhibition titled Surviving and Thriving: AIDS, Politics, and Culture; this covered medical research, the U.S. government's response, and personal stories from people with AIDS, caregivers, and activists.
Economic impact:
Main articles:
HIV/AIDS affects the economics of both individuals and countries. The gross domestic product of the most affected countries has decreased due to the lack of human capital.
Without proper nutrition, health care and medicine, large numbers of people die from AIDS-related complications. Before death they will not only be unable to work, but will also require significant medical care. It is estimated that as of 2007 there were 12 million AIDS orphans. Many are cared for by elderly grandparents.
Returning to work after beginning treatment for HIV/AIDS is difficult, and affected people often work less than the average worker. Unemployment in people with HIV/AIDS also is associated with suicidal ideation, memory problems, and social isolation.
Employment increases self-esteem, sense of dignity, confidence, and quality of life for people with HIV/AIDS. Anti-retroviral treatment may help people with HIV/AIDS work more, and may increase the chance that a person with HIV/AIDS will be employed (low-quality evidence).
By affecting mainly young adults, AIDS reduces the taxable population, in turn reducing the resources available for public expenditures such as education and health services not related to AIDS, resulting in increasing pressure on the state's finances and slower growth of the economy.
This causes a slower growth of the tax base, an effect that is reinforced if there are growing expenditures on treating the sick, training (to replace sick workers), sick pay, and caring for AIDS orphans. This is especially true if the sharp increase in adult mortality shifts the responsibility from the family to the government in caring for these orphans.
At the household level, AIDS causes both loss of income and increased spending on healthcare. A study in Côte d'Ivoire showed that households having a person with HIV/AIDS spent twice as much on medical expenses as other households. This additional expenditure also leaves less income to spend on education and other personal or family investment.
Religion and AIDS:
Main article: Religion and HIV/AIDS
The topic of religion and AIDS has become highly controversial, primarily because some religious authorities have publicly declared their opposition to the use of condoms.
The religious approach to prevent the spread of AIDS, according to a report by American health expert Matthew Hanley titled The Catholic Church and the Global AIDS Crisis, argues that cultural changes are needed, including a re-emphasis on fidelity within marriage and sexual abstinence outside of it.
Some religious organizations have claimed that prayer can cure HIV/AIDS. In 2011, the BBC reported that some churches in London were claiming that prayer would cure AIDS, and the Hackney-based Centre for the Study of Sexual Health and HIV reported that several people stopped taking their medication, sometimes on the direct advice of their pastor, leading to many deaths.
The Synagogue Church Of All Nations advertised an "anointing water" to promote God's healing, although the group denies advising people to stop taking medication.
Media portrayal:
Main article: Media portrayal of HIV/AIDS
One of the first high-profile cases of AIDS was the American gay actor Rock Hudson. He had been diagnosed during 1984, announced that he had had the virus on July 25, 1985, and died a few months later on October 2, 1985.
Another notable British casualty of AIDS that year was Nicholas Eden, a gay politician and son of former prime minister Anthony Eden.
On November 24, 1991, the virus claimed the life of British rock star Freddie Mercury, lead singer of the band Queen, who died from an AIDS-related illness having only revealed the diagnosis on the previous day.
One of the first high-profile heterosexual cases of the virus was American tennis player Arthur Ashe. He was diagnosed as HIV-positive on August 31, 1988, having contracted the virus from blood transfusions during heart surgery earlier in the 1980s. Further tests within 24 hours of the initial diagnosis revealed that Ashe had AIDS, but he did not tell the public about his diagnosis until April 1992. He died as a result on February 6, 1993, aged 49.
Therese Frare's photograph of gay activist David Kirby, as he lay dying from AIDS while surrounded by family, was taken in April 1990. Life magazine said the photo became the one image "most powerfully identified with the HIV/AIDS epidemic."
The photo was displayed in Life, was the winner of the World Press Photo, and acquired worldwide notoriety after being used in a United Colors of Benetton advertising campaign in 1992.
Many famous artists and AIDS activists such as Larry Kramer, Diamanda Galás and Rosa von Praunheim campaign for AIDS education and the rights of those affected. These artists worked with various media formats.
Criminal transmission:
Main article: Criminal transmission of HIV
Criminal transmission of HIV is the intentional or reckless infection of a person with the human immunodeficiency virus (HIV). Some countries or jurisdictions, including some areas of the United States, have laws that criminalize HIV transmission or exposure.
Others may charge the accused under laws enacted before the HIV pandemic.
In 1996, Ugandan-born Canadian Johnson Aziga was diagnosed with HIV; he subsequently had unprotected sex with eleven women without disclosing his diagnosis. By 2003, seven had contracted HIV; two died from complications related to AIDS. Aziga was convicted of first-degree murder and sentenced to life imprisonment.
Misconceptions:
Main articles:
There are many misconceptions about HIV and AIDS. Three misconceptions are that AIDS can spread through casual contact, that sexual intercourse with a virgin will cure AIDS, and that HIV can infect only gay men and drug users.
In 2014, some among the British public wrongly thought one could get HIV from kissing (16%), sharing a glass (5%), spitting (16%), a public toilet seat (4%), and coughing or sneezing (5%).
Other misconceptions are that any act of anal intercourse between two uninfected gay men can lead to HIV infection, and that open discussion of HIV and homosexuality in schools will lead to increased rates of AIDS.
A small group of individuals continue to dispute the connection between HIV and AIDS, the existence of HIV itself, or the validity of HIV testing and treatment methods. These claims, known as AIDS denialism, have been examined and rejected by the scientific community.
However, they have had a significant political impact, particularly in South Africa, where the government's official embrace of AIDS denialism (1999–2005) was responsible for its ineffective response to that country's AIDS epidemic, and has been blamed for hundreds of thousands of avoidable deaths and HIV infections.
Several discredited conspiracy theories have held that HIV was created by scientists, either inadvertently or deliberately. Operation INFEKTION was a worldwide Soviet active measures operation to spread the claim that the United States had created HIV/AIDS. Surveys show that a significant number of people believed—and continue to believe—in such claims.
At the peak of the HIV/AIDS outbreak, there was also misinformation spread from some governmental institutions. For example, Anthony Fauci, head of the National Institute of Allergy and Infectious Diseases during the AIDS outbreak, stated in the context of a conversation about childhood infections, “if the close contact of a child is a household contact, perhaps there will be a certain number of cases of individuals who are just living with and in close contact with someone with AIDS, or at risk of AIDS, who does not necessarily have to have intimate sexual contact or share a needle, but just the ordinary close contact that one sees in normal interpersonal relations.”
This and similar statements made by governmental agencies potentially fueled the unfounded fear that the public had that AIDS could be spread by ordinary close contact rather than through sexual or fluid transmission as is most commonly the case.
Research:
Main article: HIV/AIDS research
HIV/AIDS research includes all medical research which attempts to prevent, treat, or cure HIV/AIDS, along with fundamental research about the nature of HIV as an infectious agent, and about AIDS as the disease caused by HIV.
Many governments and research institutions participate in HIV/AIDS research. This research includes behavioral health interventions such as sex education, and drug development, such as research into microbicides for sexually transmitted diseases, HIV vaccines, and antiretroviral drugs.
Other medical research areas include the topics of pre-exposure prophylaxis, post-exposure prophylaxis, and circumcision and HIV. Public health officials, researchers, and programs can gain a more comprehensive picture of the barriers they face, and the efficacy of current approaches to HIV treatment and prevention, by tracking standard HIV indicators.
Use of common indicators is an increasing focus of development organizations and researchers.
See also:
Following initial infection an individual may not notice any symptoms, or may experience a brief period of influenza-like illness. Typically, this is followed by a prolonged incubation period with no symptoms.
If the infection progresses, it interferes more with the immune system, increasing the risk of developing common infections such as tuberculosis, as well as other opportunistic infections, and tumors which are rare in people who have normal immune function. These late symptoms of infection are referred to as acquired immunodeficiency syndrome (AIDS). This stage is often also associated with unintended weight loss.
HIV is spread primarily by unprotected sex (including anal and vaginal sex), contaminated hypodermic needles or blood transfusions, and from mother to child during pregnancy, delivery, or breastfeeding. Some bodily fluids, such as saliva, sweat and tears, do not transmit the virus.
Oral sex has little to no risk of transmitting the virus. Methods of prevention include:
- safe sex,
- needle exchange programs,
- treating those who are infected,
- as well as both pre- and post-exposure prophylaxis.
Disease in a baby can often be prevented by giving both the mother and child antiretroviral medication.
Recognized worldwide in the early 1980s, HIV/AIDS has had a large impact on society, both as an illness and as a source of discrimination. The disease also has large economic impacts. There are many misconceptions about HIV/AIDS, such as the belief that it can be transmitted by casual non-sexual contact.
The disease has become subject to many controversies involving religion, including the Catholic Church's position not to support condom use as prevention. It has attracted international medical and political attention as well as large-scale funding since it was identified in the 1980s.
HIV made the jump from other primates to humans in west-central Africa in the early-to-mid 20th century. AIDS was first recognized by the U.S. Centers for Disease Control and Prevention (CDC) in 1981 and its cause—HIV infection—was identified in the early part of the decade.
Between the first time AIDS was readily identified through 2021, the disease is estimated to have caused at least 40 million deaths worldwide. In 2021, there were 650,000 deaths and about 38 million people worldwide living with HIV. An estimated 20.6 million of these people live in eastern and southern Africa. HIV/AIDS is considered a pandemic—a disease outbreak which is present over a large area and is actively spreading.
The United States' National Institutes of Health (NIH) and the Gates Foundation have pledged $200 million focused on developing a global cure for AIDS. While there is no broadly available cure or vaccine, antiretroviral treatment can slow the course of the disease and may lead to a near-normal life expectancy. Treatment is recommended as soon as the diagnosis is made.
Without treatment, the average survival time after infection is 11 years.
Signs and symptoms
Main article: Signs and symptoms of HIV/AIDS
There are three main stages of HIV infection:
- acute infection,
- clinical latency,
- and AIDS.
Acute infection:
The initial period following the contraction of HIV is called acute HIV, primary HIV or acute retroviral syndrome. Many individuals develop an influenza-like illness or a mononucleosis-like illness 2–4 weeks after exposure while others have no significant symptoms.
Symptoms occur in 40–90% of cases and most commonly include:
- fever,
- large tender lymph nodes,
- throat inflammation,
- a rash,
- headache,
- tiredness,
- and/or sores of the mouth and genitals.
The rash, which occurs in 20–50% of cases, presents itself on the trunk and is maculopapular, classically.
Some people also develop opportunistic infections at this stage. Gastrointestinal symptoms, such as vomiting or diarrhea may occur. Neurological symptoms of peripheral neuropathy or Guillain–Barré syndrome also occur. The duration of the symptoms varies, but is usually one or two weeks.
Owing to their nonspecific character, these symptoms are not often recognized as signs of HIV infection. Even cases that do get seen by a family doctor or a hospital are often misdiagnosed as one of the many common infectious diseases with overlapping symptoms.
Thus, it is recommended that HIV be considered in people presenting with an unexplained fever who may have risk factors for the infection.
Clinical latency:
The initial symptoms are followed by a stage called clinical latency, asymptomatic HIV, or chronic HIV. Without treatment, this second stage of the natural history of HIV infection can last from about three years to over 20 years (on average, about eight years).
While typically there are few or no symptoms at first, near the end of this stage many people experience fever, weight loss, gastrointestinal problems and muscle pains. Between 50% and 70% of people also develop persistent generalized lymphadenopathy, characterized by unexplained, non-painful enlargement of more than one group of lymph nodes (other than in the groin) for over three to six months.
Although most HIV-1 infected individuals have a detectable viral load and in the absence of treatment will eventually progress to AIDS, a small proportion (about 5%) retain high levels of CD4+ T cells (T helper cells) without antiretroviral therapy for more than five years.
These individuals are classified as "HIV controllers" or long-term nonprogressors (LTNP). Another group consists of those who maintain a low or undetectable viral load without anti-retroviral treatment, known as "elite controllers" or "elite suppressors". They represent approximately 1 in 300 infected persons.
Acquired immunodeficiency syndrome:
Acquired immunodeficiency syndrome (AIDS) is defined as an HIV infection with either a CD4+ T cell count below 200 cells per µL or the occurrence of specific diseases associated with HIV infection. In the absence of specific treatment, around half of people infected with HIV develop AIDS within ten years.
The most common initial conditions that alert to the presence of AIDS are pneumocystis pneumonia (40%), cachexia in the form of HIV wasting syndrome (20%), and esophageal candidiasis. Other common signs include recurrent respiratory tract infections.
Opportunistic infections may be caused by bacteria, viruses, fungi, and parasites that are normally controlled by the immune system. Which infections occur depends partly on what organisms are common in the person's environment. These infections may affect nearly every organ system.
People with AIDS have an increased risk of developing various viral-induced cancers, including:
Kaposi's sarcoma is the most common cancer, occurring in 10% to 20% of people with HIV. The second-most common cancer is lymphoma, which is the cause of death of nearly 16% of people with AIDS and is the initial sign of AIDS in 3% to 4%. Both these cancers are associated with human herpesvirus 8 (HHV-8). Cervical cancer occurs more frequently in those with AIDS because of its association with human papillomavirus (HPV).
Conjunctival cancer (of the layer that lines the inner part of eyelids and the white part of the eye) is also more common in those with HIV.
Additionally, people with AIDS frequently have systemic symptoms such as prolonged fevers, sweats (particularly at night), swollen lymph nodes, chills, weakness, and unintended weight loss. Diarrhea is another common symptom, present in about 90% of people with AIDS. They can also be affected by diverse psychiatric and neurological symptoms independent of opportunistic infections and cancers.
Transmission
HIV is spread by three main routes: sexual contact, significant exposure to infected body fluids or tissues, and from mother to child during pregnancy, delivery, or breastfeeding (known as vertical transmission).
There is no risk of acquiring HIV if exposed to feces, nasal secretions, saliva, sputum, sweat, tears, urine, or vomit unless these are contaminated with blood. It is also possible to be co-infected by more than one strain of HIV—a condition known as HIV superinfection.
Sexual:
The most frequent mode of transmission of HIV is through sexual contact with an infected person. However, an HIV-positive person who has an undetectable viral load as a result of long-term treatment has effectively no risk of transmitting HIV sexually.
The existence of functionally noncontagious HIV-positive people on antiretroviral therapy was controversially publicized in the 2008 Swiss Statement, and has since become accepted as medically sound.
Globally, the most common mode of HIV transmission is via sexual contacts between people of the opposite sex; however, the pattern of transmission varies among countries. As of 2017, most HIV transmission in the United States occurred among men who had sex with men (82% of new HIV diagnoses among males aged 13 and older and 70% of total new diagnoses).
In the US, gay and bisexual men aged 13 to 24 accounted for an estimated 92% of new HIV diagnoses among all men in their age group and 27% of new diagnoses among all gay and bisexual men.
With regard to unprotected heterosexual contacts, estimates of the risk of HIV transmission per sexual act appear to be four to ten times higher in low-income countries than in high-income countries.
In low-income countries, the risk of female-to-male transmission is estimated as 0.38% per act, and of male-to-female transmission as 0.30% per act; the equivalent estimates for high-income countries are 0.04% per act for female-to-male transmission, and 0.08% per act for male-to-female transmission.
The risk of transmission from anal intercourse is especially high, estimated as 1.4–1.7% per act in both heterosexual and homosexual contacts. While the risk of transmission from oral sex is relatively low, it is still present. The risk from receiving oral sex has been described as "nearly nil"; however, a few cases have been reported. The per-act risk is estimated at 0–0.04% for receptive oral intercourse.
In settings involving prostitution in low-income countries, risk of female-to-male transmission has been estimated as 2.4% per act, and of male-to-female transmission as 0.05% per act.
Risk of transmission increases in the presence of many sexually transmitted infections and genital ulcers. Genital ulcers appear to increase the risk approximately fivefold.
Other sexually transmitted infections, such as gonorrhea, chlamydia, trichomoniasis, and bacterial vaginosis, are associated with somewhat smaller increases in risk of transmission.
The viral load of an infected person is an important risk factor in both sexual and mother-to-child transmission. During the first 2.5 months of an HIV infection a person's infectiousness is twelve times higher due to the high viral load associated with acute HIV.
If the person is in the late stages of infection, rates of transmission are approximately eightfold greater.
Commercial sex workers (including those in pornography) have an increased likelihood of contracting HIV. Rough sex can be a factor associated with an increased risk of transmission.
Sexual assault is also believed to carry an increased risk of HIV transmission as condoms are rarely worn, physical trauma to the vagina or rectum is likely, and there may be a greater risk of concurrent sexually transmitted infections.
Body fluids:
The second-most frequent mode of HIV transmission is via blood and blood products. Blood-borne transmission can be through needle-sharing during intravenous drug use, needle-stick injury, transfusion of contaminated blood or blood product, or medical injections with unsterilized equipment.
The risk from sharing a needle during drug injection is between 0.63% and 2.4% per act, with an average of 0.8%. The risk of acquiring HIV from a needle stick from an HIV-infected person is estimated as 0.3% (about 1 in 333) per act and the risk following mucous membrane exposure to infected blood as 0.09% (about 1 in 1000) per act.
This risk may, however, can be up to 5% if the introduced blood was from a person with a high viral load and the cut was deep. In the United States, intravenous drug users made up 12% of all new cases of HIV in 2009, and in some areas more than 80% of people who inject drugs are HIV-positive.
HIV is transmitted in about 90% of blood transfusions using infected blood. In developed countries the risk of acquiring HIV from a blood transfusion is extremely low (less than one in half a million) where improved donor selection and HIV screening is performed; for example, in the UK the risk is reported at one in five million and in the United States it was one in 1.5 million in 2008.
In low-income countries, only half of transfusions may be appropriately screened (as of 2008), and it is estimated that up to 15% of HIV infections in these areas come from transfusion of infected blood and blood products, representing between 5% and 10% of global infections.
It is possible to acquire HIV from organ and tissue transplantation, although this is rare because of screening.
Unsafe medical injections play a role in HIV spread in sub-Saharan Africa. In 2007, between 12% and 17% of infections in this region were attributed to medical syringe use.
The World Health Organization estimates the risk of transmission as a result of a medical injection in Africa at 1.2%. Risks are also associated with invasive procedures, assisted delivery, and dental care in this area of the world.
People giving or receiving tattoos, piercings, and scarification are theoretically at risk of infection but no confirmed cases have been documented. It is not possible for mosquitoes or other insects to transmit HIV.
Mother-to-child:
Main articles:
HIV can be transmitted from mother to child during pregnancy, during delivery, or through breast milk, resulting in the baby also contracting HIV.
As of 2008, vertical transmission accounted for about 90% of cases of HIV in children. In the absence of treatment, the risk of transmission before or during birth is around 20%, and in those who also breastfeed 35%. Treatment can decrease this risk to less than 5%.
Antiretrovirals when taken by either the mother or the baby decrease the risk of transmission in those who do breastfeed. If blood contaminates food during pre-chewing it may pose a risk of transmission.
If a woman is untreated, two years of breastfeeding results in an HIV/AIDS risk in her baby of about 17%. Due to the increased risk of death without breastfeeding in many areas in the developing world, the World Health Organization recommends either exclusive breastfeeding or the provision of safe formula.
All women known to be HIV-positive should be taking lifelong antiretroviral therapy.
Virology:
Main article: HIV
HIV is the cause of the spectrum of disease known as HIV/AIDS. HIV is a retrovirus that primarily infects components of the human immune system such as CD4+ T cells, macrophages and dendritic cells. It directly and indirectly destroys CD4+ T cells.
HIV is a member of the genus Lentivirus, part of the family Retroviridae. Lentiviruses share many morphological and biological characteristics. Many species of mammals are infected by lentiviruses, which are characteristically responsible for long-duration illnesses with a long incubation period.
Lentiviruses are transmitted as single-stranded, positive-sense, enveloped RNA viruses. Upon entry into the target cell, the viral RNA genome is converted (reverse transcribed) into double-stranded DNA by a virally encoded reverse transcriptase that is transported along with the viral genome in the virus particle.
The resulting viral DNA is then imported into the cell nucleus and integrated into the cellular DNA by a virally encoded integrase and host co-factors. Once integrated, the virus may become latent, allowing the virus and its host cell to avoid detection by the immune system.
Alternatively, the virus may be transcribed, producing new RNA genomes and viral proteins that are packaged and released from the cell as new virus particles that begin the replication cycle anew.
HIV is now known to spread between CD4+ T cells by two parallel routes: cell-free spread and cell-to-cell spread, i.e. it employs hybrid spreading mechanisms. In the cell-free spread, virus particles bud from an infected T cell, enter the blood/extracellular fluid and then infect another T cell following a chance encounter.
HIV can also disseminate by direct transmission from one cell to another by a process of cell-to-cell spread. The hybrid spreading mechanisms of HIV contribute to the virus's ongoing replication against antiretroviral therapies.
Two types of HIV have been characterized: HIV-1 and HIV-2. HIV-1 is the virus that was originally discovered (and initially referred to also as LAV or HTLV-III). It is more virulent, more infective, and is the cause of the majority of HIV infections globally. The lower infectivity of HIV-2 as compared with HIV-1 implies that fewer people exposed to HIV-2 will be infected per exposure.
Because of its relatively poor capacity for transmission, HIV-2 is largely confined to West Africa.
Pathophysiology:
Main article: Pathophysiology of HIV/AIDS
2
After the virus enters the body, there is a period of rapid viral replication, leading to an abundance of virus in the peripheral blood. During primary infection, the level of HIV may reach several million virus particles per milliliter of blood. This response is accompanied by a marked drop in the number of circulating CD4+ T cells.
The acute viremia is almost invariably associated with activation of CD8+ T cells, which kill HIV-infected cells, and subsequently with antibody production, or seroconversion. The CD8+ T cell response is thought to be important in controlling virus levels, which peak and then decline, as the CD4+ T cell counts recover. A good CD8+ T cell response has been linked to slower disease progression and a better prognosis, though it does not eliminate the virus.
Ultimately, HIV causes AIDS by depleting CD4+ T cells. This weakens the immune system and allows opportunistic infections. T cells are essential to the immune response and without them, the body cannot fight infections or kill cancerous cells.
The mechanism of CD4+ T cell depletion differs in the acute and chronic phases. During the acute phase, HIV-induced cell lysis and killing of infected cells by CD8+ T cells accounts for CD4+ T cell depletion, although apoptosis may also be a factor.
During the chronic phase, the consequences of generalized immune activation coupled with the gradual loss of the ability of the immune system to generate new T cells appear to account for the slow decline in CD4+ T cell numbers.
Although the symptoms of immune deficiency characteristic of AIDS do not appear for years after a person is infected, the bulk of CD4+ T cell loss occurs during the first weeks of infection, especially in the intestinal mucosa, which harbors the majority of the lymphocytes found in the body.
The reason for the preferential loss of mucosal CD4+ T cells is that the majority of mucosal CD4+ T cells express the CCR5 protein which HIV uses as a co-receptor to gain access to the cells, whereas only a small fraction of CD4+ T cells in the bloodstream do so.
A specific genetic change that alters the CCR5 protein when present in both chromosomes very effectively prevents HIV-1 infection.
HIV seeks out and destroys CCR5 expressing CD4+ T cells during acute infection. A vigorous immune response eventually controls the infection and initiates the clinically latent phase. CD4+ T cells in mucosal tissues remain particularly affected.
Continuous HIV replication causes a state of generalized immune activation persisting throughout the chronic phase. Immune activation, which is reflected by the increased activation state of immune cells and release of pro-inflammatory cytokines, results from the activity of several HIV gene products and the immune response to ongoing HIV replication.
It is also linked to the breakdown of the immune surveillance system of the gastrointestinal mucosal barrier caused by the depletion of mucosal CD4+ T cells during the acute phase of disease.
Diagnosis:
Main article: Diagnosis of HIV/AIDS
HIV/AIDS is diagnosed via laboratory testing and then staged based on the presence of certain signs or symptoms. HIV screening is recommended by the United States Preventive Services Task Force for all people 15 years to 65 years of age, including all pregnant women.
Additionally, testing is recommended for those at high risk, which includes anyone diagnosed with a sexually transmitted illness. In many areas of the world, a third of HIV carriers only discover they are infected at an advanced stage of the disease when AIDS or severe immunodeficiency has become apparent.
HIV testing:
Most people infected with HIV develop specific antibodies (i.e. seroconvert) within three to twelve weeks after the initial infection. Diagnosis of primary HIV before seroconversion is done by measuring HIV-RNA or p24 antigen. Positive results obtained by antibody or PCR testing are confirmed either by a different antibody or by PCR.
Antibody tests in children younger than 18 months are typically inaccurate, due to the continued presence of maternal antibodies. Thus HIV infection can only be diagnosed by PCR testing for HIV RNA or DNA, or via testing for the p24 antigen. Much of the world lacks access to reliable PCR testing, and people in many places simply wait until either symptoms develop or the child is old enough for accurate antibody testing.
In sub-Saharan Africa between 2007 and 2009, between 30% and 70% of the population were aware of their HIV status. In 2009, between 3.6% and 42% of men and women in sub-Saharan countries were tested; this represented a significant increase compared to previous years.
Classifications:
Two main clinical staging systems are used to classify HIV and HIV-related disease for surveillance purposes: the WHO disease staging system for HIV infection and disease, and the CDC classification system for HIV infection. The CDC's classification system is more frequently adopted in developed countries.
Since the WHO's staging system does not require laboratory tests, it is suited to the resource-restricted conditions encountered in developing countries, where it can also be used to help guide clinical management. Despite their differences, the two systems allow a comparison for statistical purposes.
The World Health Organization first proposed a definition for AIDS in 1986. Since then, the WHO classification has been updated and expanded several times, with the most recent version being published in 2007.
The WHO system uses the following categories:
- Primary HIV infection: May be either asymptomatic or associated with acute retroviral syndrome
- Stage I: HIV infection is asymptomatic with a CD4+ T cell count (also known as CD4 count) greater than 500 per microlitre (µl or cubic mm) of blood. May include generalized lymph node enlargement.
- Stage II: Mild symptoms, which may include minor mucocutaneous manifestations and recurrent upper respiratory tract infections. A CD4 count of less than 500/µl
- Stage III: Advanced symptoms, which may include unexplained chronic diarrhea for longer than a month, severe bacterial infections including tuberculosis of the lung, and a CD4 count of less than 350/µl
- Stage IV or AIDS: severe symptoms, which include toxoplasmosis of the brain, candidiasis of the esophagus, trachea, bronchi, or lungs, and Kaposi's sarcoma. A CD4 count of less than 200/µl.
The U.S. Centers for Disease Control and Prevention also created a classification system for HIV, and updated it in 2008 and 2014. This system classifies HIV infections based on CD4 count and clinical symptoms, and describes the infection in five groups. In those greater than six years of age it is:
- Stage 0: the time between a negative or indeterminate HIV test followed less than 180 days by a positive test.
- Stage 1: CD4 count ≥ 500 cells/µl and no AIDS-defining conditions.
- Stage 2: CD4 count 200 to 500 cells/µl and no AIDS-defining conditions.
- Stage 3: CD4 count ≤ 200 cells/µl or AIDS-defining conditions.
- Unknown: if insufficient information is available to make any of the above classifications.
For surveillance purposes, the AIDS diagnosis still stands even if, after treatment, the CD4+ T cell count rises to above 200 per µL of blood or other AIDS-defining illnesses are cured.
Prevention:
Main article: Prevention of HIV/AIDS
Sexual Contact:
Consistent condom use reduces the risk of HIV transmission by approximately 80% over the long term. When condoms are used consistently by a couple in which one person is infected, the rate of HIV infection is less than 1% per year.
There is some evidence to suggest that female condoms may provide an equivalent level of protection.
Application of a vaginal gel containing tenofovir (a reverse transcriptase inhibitor) immediately before sex seems to reduce infection rates by approximately 40% among African women.
By contrast, use of the spermicide nonoxynol-9 may increase the risk of transmission due to its tendency to cause vaginal and rectal irritation.
Circumcision in sub-Saharan Africa "reduces the acquisition of HIV by heterosexual men by between 38% and 66% over 24 months". Owing to these studies, both the World Health Organization and UNAIDS recommended male circumcision in 2007 as a method of preventing female-to-male HIV transmission in areas with high rates of HIV.
However, whether it protects against male-to-female transmission is disputed, and whether it is of benefit in developed countries and among men who have sex with men is undetermined.
Programs encouraging sexual abstinence do not appear to affect subsequent HIV risk.
Evidence of any benefit from peer education is equally poor. Comprehensive sexual education provided at school may decrease high-risk behavior.
A substantial minority of young people continues to engage in high-risk practices despite knowing about HIV/AIDS, underestimating their own risk of becoming infected with HIV.
Voluntary counseling and testing people for HIV does not affect risky behavior in those who test negative but does increase condom use in those who test positive. Enhanced family planning services appear to increase the likelihood of women with HIV using contraception, compared to basic services. It is not known whether treating other sexually transmitted infections is effective in preventing HIV.
Pre-exposure:
Antiretroviral treatment among people with HIV whose CD4 count ≤ 550 cells/µL is a very effective way to prevent HIV infection of their partner (a strategy known as treatment as prevention, or TASP). TASP is associated with a 10- to 20-fold reduction in transmission risk.
Pre-exposure prophylaxis (PrEP) with a daily dose of the medications tenofovir, with or without emtricitabine, is effective in people at high risk including men who have sex with men, couples where one is HIV-positive, and young heterosexuals in Africa. It may also be effective in intravenous drug users, with a study finding a decrease in risk of 0.7 to 0.4 per 100 person years. The USPSTF, in 2019, recommended PrEP in those who are at high risk.
Universal precautions within the health care environment are believed to be effective in decreasing the risk of HIV. Intravenous drug use is an important risk factor, and harm reduction strategies such as needle-exchange programs and opioid substitution therapy appear effective in decreasing this risk.
Post-exposure:
A course of antiretrovirals administered within 48 to 72 hours after exposure to HIV-positive blood or genital secretions is referred to as post-exposure prophylaxis (PEP). The use of the single agent zidovudine reduces the risk of a HIV infection five-fold following a needle-stick injury.
As of 2013, the prevention regimen recommended in the United States consists of three medications--tenofovir, emtricitabine and raltegravir—as this may reduce the risk further.
PEP treatment is recommended after a sexual assault when the perpetrator is known to be HIV-positive, but is controversial when their HIV status is unknown. The duration of treatment is usually four weeks and is frequently associated with adverse effects—where zidovudine is used, about 70% of cases result in adverse effects such as nausea (24%), fatigue (22%), emotional distress (13%) and headaches (9%).
Mother-to-child:
Main article: HIV and pregnancy
Programs to prevent the vertical transmission of HIV (from mothers to children) can reduce rates of transmission by 92–99%. This primarily involves the use of a combination of antiviral medications during pregnancy and after birth in the infant, and potentially includes bottle feeding rather than breastfeeding.
If replacement feeding is acceptable, feasible, affordable, sustainable and safe, mothers should avoid breastfeeding their infants; however, exclusive breastfeeding is recommended during the first months of life if this is not the case. If exclusive breastfeeding is carried out, the provision of extended antiretroviral prophylaxis to the infant decreases the risk of transmission.
In 2015, Cuba became the first country in the world to eradicate mother-to-child transmission of HIV.
Vaccination:
Main article: HIV vaccine
Currently there is no licensed vaccine for HIV or AIDS.The most effective vaccine trial to date, RV 144, was published in 2009; it found a partial reduction in the risk of transmission of roughly 30%, stimulating some hope in the research community of developing a truly effective vaccine.
Treatment:
Main article: Management of HIV/AIDS
There is currently no cure, nor an effective HIV vaccine. Treatment consists of highly active antiretroviral therapy (HAART), which slows progression of the disease. As of 2010, more than 6.6 million people were receiving HAART in low- and middle-income countries.
Treatment also includes preventive and active treatment of opportunistic infections. As of July 2022, four people have been successfully cleared of HIV. Rapid initiation of antiretroviral therapy within one week of diagnosis appear to improve treatment outcomes in low and medium-income settings.
Antiviral therapy:
Current HAART options are combinations (or "cocktails") consisting of at least three medications belonging to at least two types, or "classes", of antiretroviral agents.
Initially, treatment is typically a non-nucleoside reverse transcriptase inhibitor (NNRTI) plus two nucleoside analog reverse transcriptase inhibitors (NRTIs). Typical NRTIs include: zidovudine (AZT) or tenofovir (TDF) and lamivudine (3TC) or emtricitabine (FTC).
As of 2019, dolutegravir/lamivudine/tenofovir is listed by the World Health Organization as the first-line treatment for adults, with tenofovir/lamivudine/efavirenz as an alternative.
Combinations of agents that include protease inhibitors (PI) are used if the above regimen loses effectiveness.
The World Health Organization and the United States recommend antiretrovirals in people of all ages (including pregnant women) as soon as the diagnosis is made, regardless of CD4 count. Once treatment is begun, it is recommended that it is continued without breaks or "holidays".
Many people are diagnosed only after treatment ideally should have begun. The desired outcome of treatment is a long-term plasma HIV-RNA count below 50 copies/mL. Levels to determine if treatment is effective are initially recommended after four weeks and once levels fall below 50 copies/mL checks every three to six months are typically adequate.
Inadequate control is deemed to be greater than 400 copies/mL. Based on these criteria treatment is effective in more than 95% of people during the first year.
Benefits of treatment include a decreased risk of progression to AIDS and a decreased risk of death. In the developing world, treatment also improves physical and mental health.
With treatment, there is a 70% reduced risk of acquiring tuberculosis. Additional benefits include a decreased risk of transmission of the disease to sexual partners and a decrease in mother-to-child transmission.
The effectiveness of treatment depends to a large part on compliance. Reasons for non-adherence to treatment include poor access to medical care, inadequate social supports, mental illness and drug abuse. The complexity of treatment regimens (due to pill numbers and dosing frequency) and adverse effects may reduce adherence.
Even though cost is an important issue with some medications, 47% of those who needed them were taking them in low- and middle-income countries as of 2010, and the rate of adherence is similar in low-income and high-income countries.
Specific adverse events are related to the antiretroviral agent taken. Some relatively common adverse events include: lipodystrophy syndrome, dyslipidemia, and diabetes mellitus, especially with protease inhibitors.
Other common symptoms include diarrhea, and an increased risk of cardiovascular disease. Newer recommended treatments are associated with fewer adverse effects. Certain medications may be associated with birth defects and therefore may be unsuitable for women hoping to have children.
Treatment recommendations for children are somewhat different from those for adults. The World Health Organization recommends treating all children less than five years of age; children above five are treated like adults.
The United States guidelines recommend treating all children less than 12 months of age and all those with HIV RNA counts greater than 100,000 copies/mL between one year and five years of age.
The European Medicines Agency (EMA) has recommended the granting of marketing authorizations for two new antiretroviral (ARV) medicines, rilpivirine (Rekambys) and cabotegravir (Vocabria), to be used together for the treatment of people with human immunodeficiency virus type 1 (HIV-1) infection.
The two medicines are the first ARVs that come in a long-acting injectable formulation. This means that instead of daily pills, people receive intramuscular injections monthly or every two months.
The combination of Rekambys and Vocabria injection is intended for maintenance treatment of adults who have undetectable HIV levels in the blood (viral load less than 50 copies/ml) with their current ARV treatment, and when the virus has not developed resistance to a certain class of anti-HIV medicines called non-nucleoside reverse transcriptase inhibitors (NNRTIs) and integrase strand transfer inhibitors (INIs).
Cabotegravir combined with rilpivirine (Cabenuva) is a complete regimen for the treatment of human immunodeficiency virus type 1 (HIV-1) infection in adults to replace a current antiretroviral regimen in those who are virologically suppressed on a stable antiretroviral regimen with no history of treatment failure and with no known or suspected resistance to either cabotegravir or rilpivirine.
Opportunistic infections:
Main article: Opportunistic infection § Opportunistic Infection and HIV/AIDS
Measures to prevent opportunistic infections are effective in many people with HIV/AIDS. In addition to improving current disease, treatment with antiretrovirals reduces the risk of developing additional opportunistic infections.
Adults and adolescents who are living with HIV (even on anti-retroviral therapy) with no evidence of active tuberculosis in settings with high tuberculosis burden should receive isoniazid preventive therapy (IPT); the tuberculin skin test can be used to help decide if IPT is needed.
Children with HIV may benefit from screening for tuberculosis.
Vaccination against hepatitis A and B is advised for all people at risk of HIV before they become infected; however, it may also be given after infection.
Trimethoprim/sulfamethoxazole prophylaxis between four and six weeks of age, and ceasing breastfeeding of infants born to HIV-positive mothers, is recommended in resource-limited settings. It is also recommended to prevent PCP when a person's CD4 count is below 200 cells/uL and in those who have or have previously had PCP.
People with substantial immunosuppression are also advised to receive prophylactic therapy for toxoplasmosis and MAC. Appropriate preventive measures reduced the rate of these infections by 50% between 1992 and 1997. Influenza vaccination and pneumococcal polysaccharide vaccine are often recommended in people with HIV/AIDS with some evidence of benefit.
Diet:
Main article: Nutrition and HIV/AIDS
The World Health Organization (WHO) has issued recommendations regarding nutrient requirements in HIV/AIDS. A generally healthy diet is promoted. Dietary intake of micronutrients at RDA levels by HIV-infected adults is recommended by the WHO; higher intake of vitamin A, zinc, and iron can produce adverse effects in HIV-positive adults, and is not recommended unless there is documented deficiency.
Dietary supplementation for people who are infected with HIV and who have inadequate nutrition or dietary deficiencies may strengthen their immune systems or help them recover from infections; however, evidence indicating an overall benefit in morbidity or reduction in mortality is not consistent.
People with HIV/AIDS are up to four times more likely to develop type 2 diabetes than those who are not tested positive with the virus.
Evidence for supplementation with selenium is mixed with some tentative evidence of benefit. For pregnant and lactating women with HIV, multivitamin supplement improves outcomes for both mothers and children. If the pregnant or lactating mother has been advised to take anti-retroviral medication to prevent mother-to-child HIV transmission, multivitamin supplements should not replace these treatments.
There is some evidence that vitamin A supplementation in children with an HIV infection reduces mortality and improves growth.
Alternative medicine:
In the US, approximately 60% of people with HIV use various forms of complementary or alternative medicine, whose effectiveness has not been established. There is not enough evidence to support the use of herbal medicines. There is insufficient evidence to recommend or support the use of medical cannabis to try to increase appetite or weight gain.
Prognosis:
HIV/AIDS has become a chronic rather than an acutely fatal disease in many areas of the world. Prognosis varies between people, and both the CD4 count and viral load are useful for predicted outcomes.
Without treatment, average survival time after infection with HIV is estimated to be 9 to 11 years, depending on the HIV subtype. After the diagnosis of AIDS, if treatment is not available, survival ranges between 6 and 19 months.
HAART and appropriate prevention of opportunistic infections reduces the death rate by 80%, and raises the life expectancy for a newly diagnosed young adult to 20–50 years. This is between two thirds and nearly that of the general population.
If treatment is started late in the infection, prognosis is not as good: for example, if treatment is begun following the diagnosis of AIDS, life expectancy is ~10–40 years. Half of infants born with HIV die before two years of age without treatment.
The primary causes of death from HIV/AIDS are opportunistic infections and cancer, both of which are frequently the result of the progressive failure of the immune system.Risk of cancer appears to increase once the CD4 count is below 500/μL.
The rate of clinical disease progression varies widely between individuals and has been shown to be affected by a number of factors such as:
- a person's susceptibility and immune function;
- their access to health care,
- the presence of co-infections;
- and the particular strain (or strains) of the virus involved.
Tuberculosis co-infection is one of the leading causes of sickness and death in those with HIV/AIDS being present in a third of all HIV-infected people and causing 25% of HIV-related deaths.
HIV is also one of the most important risk factors for tuberculosis. Hepatitis C is another very common co-infection where each disease increases the progression of the other.
The two most common cancers associated with HIV/AIDS are Kaposi's sarcoma and AIDS-related non-Hodgkin's lymphoma. Other cancers that are more frequent include:
Even with anti-retroviral treatment, over the long term HIV-infected people may experience:
Some conditions, such as lipodystrophy, may be caused both by HIV and its treatment.
Epidemiology:
Main article: Epidemiology of HIV/AIDS
Some authors consider HIV/AIDS a global pandemic. As of 2016, approximately 36.7 million people worldwide have HIV, the number of new infections that year being about 1.8 million. This is down from 3.1 million new infections in 2001. Slightly over half the infected population are women and 2.1 million are children. It resulted in about 1 million deaths in 2016, down from a peak of 1.9 million in 2005.
Sub-Saharan Africa is the region most affected. In 2010, an estimated 68% (22.9 million) of all HIV cases and 66% of all deaths (1.2 million) occurred in this region. This means that about 5% of the adult population is infected and it is believed to be the cause of 10% of all deaths in children.
Here, in contrast to other regions, women comprise nearly 60% of cases. South Africa has the largest population of people with HIV of any country in the world at 5.9 million.
Life expectancy has fallen in the worst-affected countries due to HIV/AIDS; for example, in 2006 it was estimated that it had dropped from 65 to 35 years in Botswana. Mother-to-child transmission in Botswana and South Africa, as of 2013, has decreased to less than 5%, with improvement in many other African nations due to improved access to antiretroviral therapy.
South & South East Asia is the second most affected; in 2010 this region contained an estimated 4 million cases or 12% of all people living with HIV resulting in approximately 250,000 deaths. Approximately 2.4 million of these cases are in India.
During 2008 in the United States approximately 1.2 million people aged ≥13 years were living with HIV, resulting in about 17,500 deaths. The US Centers for Disease Control and Prevention estimated that in that year, 236,400 people or 20% of infected Americans were unaware of their infection.
As of 2016 about 675,000 people have died of HIV/AIDS in the US since the beginning of the HIV epidemic. In the United Kingdom as of 2015, there were approximately 101,200 cases which resulted in 594 deaths.
In Canada as of 2008, there were about 65,000 cases causing 53 deaths. Between the first recognition of AIDS (in 1981) and 2009, it has led to nearly 30 million deaths. Rates of HIV are lowest in North Africa and the Middle East (0.1% or less), East Asia (0.1%), and Western and Central Europe (0.2%).
The worst-affected European countries, in 2009 and 2012 estimates, are Russia, Ukraine, Latvia, Moldova, Portugal and Belarus, in decreasing order of prevalence.
History:
Main article: History of HIV/AIDS
- For a chronological guide, see Timeline of HIV/AIDS.
- Further information: Category:HIV/AIDS by country
Discovery:
The first news story on the disease appeared on May 18, 1981, in the gay newspaper New York Native.
AIDS was first clinically reported on June 5, 1981, with five cases in the United States. The initial cases were a cluster of injecting drug users and gay men with no known cause of impaired immunity who showed symptoms of Pneumocystis carinii pneumonia (PCP), a rare opportunistic infection that was known to occur in people with very compromised immune systems.
Soon thereafter, a large number of homosexual men developed a generally rare skin cancer called Kaposi's sarcoma (KS). Many more cases of PCP and KS emerged, alerting U.S. Centers for Disease Control and Prevention (CDC) and a CDC task force was formed to monitor the outbreak.
In the early days, the CDC did not have an official name for the disease, often referring to it by way of diseases associated with it, such as lymphadenopathy, the disease after which the discoverers of HIV originally named the virus.
They also used Kaposi's sarcoma and opportunistic infections, the name by which a task force had been set up in 1981. At one point the CDC referred to it as the "4H disease", as the syndrome seemed to affect heroin users, homosexuals, hemophiliacs, and Haitians.
The term GRID, which stood for gay-related immune deficiency, had also been coined. However, after determining that AIDS was not isolated to the gay community, it was realized that the term GRID was misleading, and the term AIDS was introduced at a meeting in July 1982.
By September 1982 the CDC started referring to the disease as AIDS.
In 1983, two separate research groups led by Robert Gallo and Luc Montagnier declared that a novel retrovirus may have been infecting people with AIDS, and published their findings in the same issue of the journal Science.
Gallo claimed a virus which his group had isolated from a person with AIDS was strikingly similar in shape to other human T-lymphotropic viruses (HTLVs) that his group had been the first to isolate. Gallo's group called their newly isolated virus HTLV-III.
At the same time, Montagnier's group isolated a virus from a person presenting with swelling of the lymph nodes of the neck and physical weakness, two characteristic symptoms of AIDS.
Contradicting the report from Gallo's group, Montagnier and his colleagues showed that core proteins of this virus were immunologically different from those of HTLV-I. Montagnier's group named their isolated virus lymphadenopathy-associated virus (LAV).
As these two viruses turned out to be the same, in 1986, LAV and HTLV-III were renamed HIV.
Origins:
The origin of HIV / AIDS and the circumstances that led to its emergence remain unsolved.
Both HIV-1 and HIV-2 are believed to have originated in non-human primates in West-central Africa and were transferred to humans in the early 20th century.
HIV-1 appears to have originated in southern Cameroon through the evolution of SIV(cpz), a simian immunodeficiency virus (SIV) that infects wild chimpanzees (HIV-1 descends from the SIVcpz endemic in the chimpanzee subspecies Pan troglodytes troglodytes).
The closest relative of HIV-2 is SIV (smm), a virus of the sooty mangabey (Cercocebus atys atys), an Old World monkey living in coastal West Africa (from southern Senegal to western Ivory Coast).
New World monkeys such as the owl monkey are resistant to HIV-1 infection, possibly because of a genomic fusion of two viral resistance genes. HIV-1 is thought to have jumped the species barrier on at least three separate occasions, giving rise to the three groups of the virus, M, N, and O.
There is evidence that humans who participate in bushmeat activities, either as hunters or as bushmeat vendors, commonly acquire SIV. However, SIV is a weak virus which is typically suppressed by the human immune system within weeks of infection.
It is thought that several transmissions of the virus from individual to individual in quick succession are necessary to allow it enough time to mutate into HIV.
Furthermore, due to its relatively low person-to-person transmission rate, SIV can only spread throughout the population in the presence of one or more high-risk transmission channels, which are thought to have been absent in Africa before the 20th century.
Specific proposed high-risk transmission channels, allowing the virus to adapt to humans and spread throughout society, depend on the proposed timing of the animal-to-human crossing.
Genetic studies of the virus suggest that the most recent common ancestor of the HIV-1 M group dates back to c. 1910. Proponents of this dating link the HIV epidemic with the emergence of colonialism and growth of large colonial African cities, leading to social changes, including a higher degree of sexual promiscuity, the spread of prostitution, and the accompanying high frequency of genital ulcer diseases (such as syphilis) in nascent colonial cities.
While transmission rates of HIV during vaginal intercourse are low under regular circumstances, they are increased manyfold if one of the partners has a sexually transmitted infection causing genital ulcers. Early 1900s colonial cities were notable for their high prevalence of prostitution and genital ulcers, to the degree that, as of 1928, as many as 45% of female residents of eastern Kinshasa were thought to have been prostitutes, and, as of 1933, around 15% of all residents of the same city had syphilis.
An alternative view holds that unsafe medical practices in Africa after World War II, such as unsterile reuse of single-use syringes during mass vaccination, antibiotic and anti-malaria treatment campaigns, were the initial vector that allowed the virus to adapt to humans and spread.
The earliest well-documented case of HIV in a human dates back to 1959 in the Congo. The virus may have been present in the U.S. as early as the mid-to-late 1950s, as a sixteen-year-old male named Robert Rayford presented with symptoms in 1966 and died in 1969. In the 1970s, there were cases of getting parasites and becoming sick with what was called "gay bowel disease", but what is now suspected to have been AIDS.
The earliest retrospectively described case of AIDS is believed to have been in Norway beginning in 1966, that of Arvid Noe. In July 1960, in the wake of Congo's independence, the United Nations recruited Francophone experts and technicians from all over the world to assist in filling administrative gaps left by Belgium, who did not leave behind an African elite to run the country.
By 1962, Haitians made up the second-largest group of well-educated experts (out of the 48 national groups recruited), that totaled around 4500 in the country. Dr. Jacques Pépin, a Canadian author of The Origins of AIDS, stipulates that Haiti was one of HIV's entry points to the U.S. and that a Haitian may have carried HIV back across the Atlantic in the 1960s.
Although there was known to have been at least one case of AIDS in the U.S. from 1966, the vast majority of infections occurring outside sub-Saharan Africa (including the U.S.) can be traced back to a single unknown individual who became infected with HIV in Haiti and brought the infection to the U.S. at some time around 1969. The epidemic rapidly spread among high-risk groups (initially, sexually promiscuous men who have sex with men).
By 1978, the prevalence of HIV-1 among gay male residents of New York City and San Francisco was estimated at 5%, suggesting that several thousand individuals in the country had been infected.
Society and culture
Stigma:
Main article: Discrimination against people with HIV/AIDS
AIDS stigma exists around the world in a variety of ways, including:
- ostracism,
- rejection,
- discrimination and avoidance of HIV-infected people;
- compulsory HIV testing without prior consent or protection of confidentiality;
- violence against HIV-infected individuals or people who are perceived to be infected with HIV;
- and the quarantine of HIV-infected individuals.
Stigma-related violence or the fear of violence prevents many people from seeking HIV testing, returning for their results, or securing treatment, possibly turning what could be a manageable chronic illness into a death sentence and perpetuating the spread of HIV.
AIDS stigma has been further divided into the following three categories:
- Instrumental AIDS stigma—a reflection of the fear and apprehension that are likely to be associated with any deadly and transmissible illness.
- Symbolic AIDS stigma—the use of HIV/AIDS to express attitudes toward the social groups or lifestyles perceived to be associated with the disease.
- Courtesy AIDS stigma—stigmatization of people connected to the issue of HIV/AIDS or HIV-positive people.
Often, AIDS stigma is expressed in conjunction with one or more other stigmas, particularly those associated with homosexuality, bisexuality, promiscuity, prostitution, and intravenous drug use.
In many developed countries, there is an association between AIDS and homosexuality or bisexuality, and this association is correlated with higher levels of sexual prejudice, such as anti-homosexual or anti-bisexual attitudes.
There is also a perceived association between AIDS and all male-male sexual behavior, including sex between uninfected men. However, the dominant mode of spread worldwide for HIV remains heterosexual transmission.
To get a better understanding of the anti-homosexual attitudes around AIDs the musical Rent explores this.
In 2003, as part of an overall reform of marriage and population legislation, it became legal for those diagnosed with AIDS to marry in China.
In 2013, the U.S. National Library of Medicine developed a traveling exhibition titled Surviving and Thriving: AIDS, Politics, and Culture; this covered medical research, the U.S. government's response, and personal stories from people with AIDS, caregivers, and activists.
Economic impact:
Main articles:
HIV/AIDS affects the economics of both individuals and countries. The gross domestic product of the most affected countries has decreased due to the lack of human capital.
Without proper nutrition, health care and medicine, large numbers of people die from AIDS-related complications. Before death they will not only be unable to work, but will also require significant medical care. It is estimated that as of 2007 there were 12 million AIDS orphans. Many are cared for by elderly grandparents.
Returning to work after beginning treatment for HIV/AIDS is difficult, and affected people often work less than the average worker. Unemployment in people with HIV/AIDS also is associated with suicidal ideation, memory problems, and social isolation.
Employment increases self-esteem, sense of dignity, confidence, and quality of life for people with HIV/AIDS. Anti-retroviral treatment may help people with HIV/AIDS work more, and may increase the chance that a person with HIV/AIDS will be employed (low-quality evidence).
By affecting mainly young adults, AIDS reduces the taxable population, in turn reducing the resources available for public expenditures such as education and health services not related to AIDS, resulting in increasing pressure on the state's finances and slower growth of the economy.
This causes a slower growth of the tax base, an effect that is reinforced if there are growing expenditures on treating the sick, training (to replace sick workers), sick pay, and caring for AIDS orphans. This is especially true if the sharp increase in adult mortality shifts the responsibility from the family to the government in caring for these orphans.
At the household level, AIDS causes both loss of income and increased spending on healthcare. A study in Côte d'Ivoire showed that households having a person with HIV/AIDS spent twice as much on medical expenses as other households. This additional expenditure also leaves less income to spend on education and other personal or family investment.
Religion and AIDS:
Main article: Religion and HIV/AIDS
The topic of religion and AIDS has become highly controversial, primarily because some religious authorities have publicly declared their opposition to the use of condoms.
The religious approach to prevent the spread of AIDS, according to a report by American health expert Matthew Hanley titled The Catholic Church and the Global AIDS Crisis, argues that cultural changes are needed, including a re-emphasis on fidelity within marriage and sexual abstinence outside of it.
Some religious organizations have claimed that prayer can cure HIV/AIDS. In 2011, the BBC reported that some churches in London were claiming that prayer would cure AIDS, and the Hackney-based Centre for the Study of Sexual Health and HIV reported that several people stopped taking their medication, sometimes on the direct advice of their pastor, leading to many deaths.
The Synagogue Church Of All Nations advertised an "anointing water" to promote God's healing, although the group denies advising people to stop taking medication.
Media portrayal:
Main article: Media portrayal of HIV/AIDS
One of the first high-profile cases of AIDS was the American gay actor Rock Hudson. He had been diagnosed during 1984, announced that he had had the virus on July 25, 1985, and died a few months later on October 2, 1985.
Another notable British casualty of AIDS that year was Nicholas Eden, a gay politician and son of former prime minister Anthony Eden.
On November 24, 1991, the virus claimed the life of British rock star Freddie Mercury, lead singer of the band Queen, who died from an AIDS-related illness having only revealed the diagnosis on the previous day.
One of the first high-profile heterosexual cases of the virus was American tennis player Arthur Ashe. He was diagnosed as HIV-positive on August 31, 1988, having contracted the virus from blood transfusions during heart surgery earlier in the 1980s. Further tests within 24 hours of the initial diagnosis revealed that Ashe had AIDS, but he did not tell the public about his diagnosis until April 1992. He died as a result on February 6, 1993, aged 49.
Therese Frare's photograph of gay activist David Kirby, as he lay dying from AIDS while surrounded by family, was taken in April 1990. Life magazine said the photo became the one image "most powerfully identified with the HIV/AIDS epidemic."
The photo was displayed in Life, was the winner of the World Press Photo, and acquired worldwide notoriety after being used in a United Colors of Benetton advertising campaign in 1992.
Many famous artists and AIDS activists such as Larry Kramer, Diamanda Galás and Rosa von Praunheim campaign for AIDS education and the rights of those affected. These artists worked with various media formats.
Criminal transmission:
Main article: Criminal transmission of HIV
Criminal transmission of HIV is the intentional or reckless infection of a person with the human immunodeficiency virus (HIV). Some countries or jurisdictions, including some areas of the United States, have laws that criminalize HIV transmission or exposure.
Others may charge the accused under laws enacted before the HIV pandemic.
In 1996, Ugandan-born Canadian Johnson Aziga was diagnosed with HIV; he subsequently had unprotected sex with eleven women without disclosing his diagnosis. By 2003, seven had contracted HIV; two died from complications related to AIDS. Aziga was convicted of first-degree murder and sentenced to life imprisonment.
Misconceptions:
Main articles:
There are many misconceptions about HIV and AIDS. Three misconceptions are that AIDS can spread through casual contact, that sexual intercourse with a virgin will cure AIDS, and that HIV can infect only gay men and drug users.
In 2014, some among the British public wrongly thought one could get HIV from kissing (16%), sharing a glass (5%), spitting (16%), a public toilet seat (4%), and coughing or sneezing (5%).
Other misconceptions are that any act of anal intercourse between two uninfected gay men can lead to HIV infection, and that open discussion of HIV and homosexuality in schools will lead to increased rates of AIDS.
A small group of individuals continue to dispute the connection between HIV and AIDS, the existence of HIV itself, or the validity of HIV testing and treatment methods. These claims, known as AIDS denialism, have been examined and rejected by the scientific community.
However, they have had a significant political impact, particularly in South Africa, where the government's official embrace of AIDS denialism (1999–2005) was responsible for its ineffective response to that country's AIDS epidemic, and has been blamed for hundreds of thousands of avoidable deaths and HIV infections.
Several discredited conspiracy theories have held that HIV was created by scientists, either inadvertently or deliberately. Operation INFEKTION was a worldwide Soviet active measures operation to spread the claim that the United States had created HIV/AIDS. Surveys show that a significant number of people believed—and continue to believe—in such claims.
At the peak of the HIV/AIDS outbreak, there was also misinformation spread from some governmental institutions. For example, Anthony Fauci, head of the National Institute of Allergy and Infectious Diseases during the AIDS outbreak, stated in the context of a conversation about childhood infections, “if the close contact of a child is a household contact, perhaps there will be a certain number of cases of individuals who are just living with and in close contact with someone with AIDS, or at risk of AIDS, who does not necessarily have to have intimate sexual contact or share a needle, but just the ordinary close contact that one sees in normal interpersonal relations.”
This and similar statements made by governmental agencies potentially fueled the unfounded fear that the public had that AIDS could be spread by ordinary close contact rather than through sexual or fluid transmission as is most commonly the case.
Research:
Main article: HIV/AIDS research
HIV/AIDS research includes all medical research which attempts to prevent, treat, or cure HIV/AIDS, along with fundamental research about the nature of HIV as an infectious agent, and about AIDS as the disease caused by HIV.
Many governments and research institutions participate in HIV/AIDS research. This research includes behavioral health interventions such as sex education, and drug development, such as research into microbicides for sexually transmitted diseases, HIV vaccines, and antiretroviral drugs.
Other medical research areas include the topics of pre-exposure prophylaxis, post-exposure prophylaxis, and circumcision and HIV. Public health officials, researchers, and programs can gain a more comprehensive picture of the barriers they face, and the efficacy of current approaches to HIV treatment and prevention, by tracking standard HIV indicators.
Use of common indicators is an increasing focus of development organizations and researchers.
See also:
- HIV/AIDS at Curlie
- UNAIDS – Joint United Nations Program on HIV/AIDS
- HIVinfo – Information on HIV/AIDS treatment, prevention, and research, U.S. Department of Health and Human Services
- 2018 Recommendations of the International Antiviral Society